Anatomy of the Eye
Familiarize yourself with the sagittal (vertical cross sectional) diagram of the eye ball below.
Picture_Human Eye (Sagittal) Cross Section
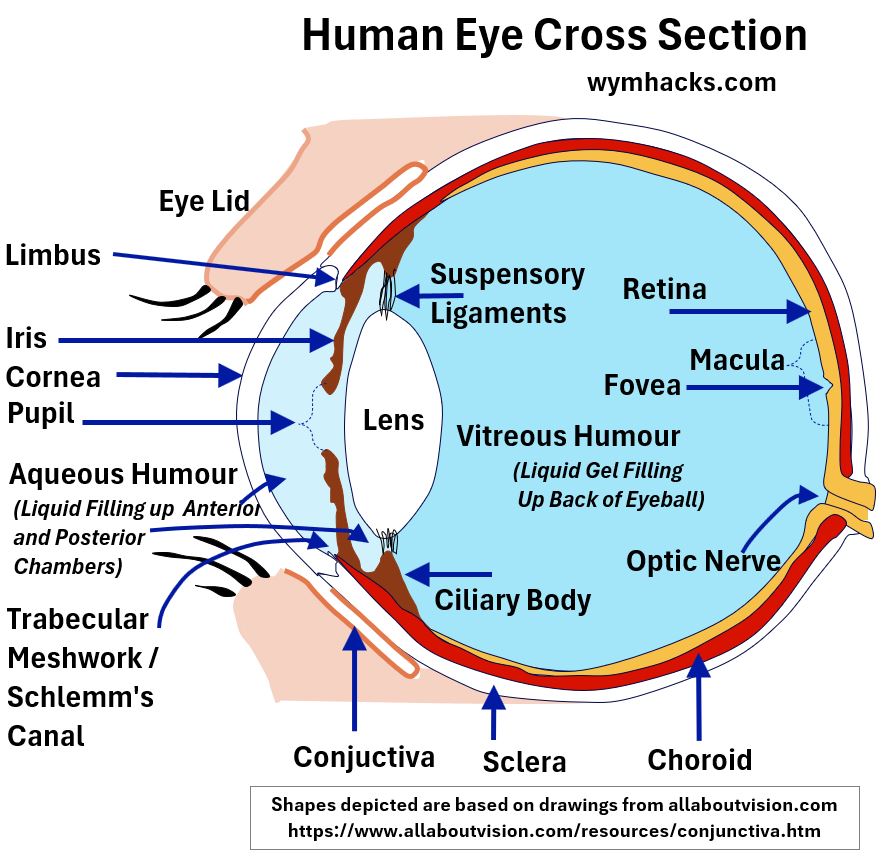
Imagine an object that you are seeing to the left of the drawing above.
Light rays from the object enter the eye and are refracted by the Cornea (mainly) , the Lens, and the media in between.
These refractive media, as a composite, behave like a converging biconvex lens.
- For more on lenses, see my article Lens Ray Diagrams.
- Also see my article Eye Anatomy
In a “clear seeing eye”, an object’s light converges towards the central axis of the eyeball and projects onto the back of the eye.
- The back inner layer of the eyeball, the Retina, receives an inverted image of the object.
- The image will land on the Fovea, the most sensitive light sensing region of the Retina.
- Light converts to electric signals in the Retina, which then move down the optic nerve and are converted by the Brain into vision.
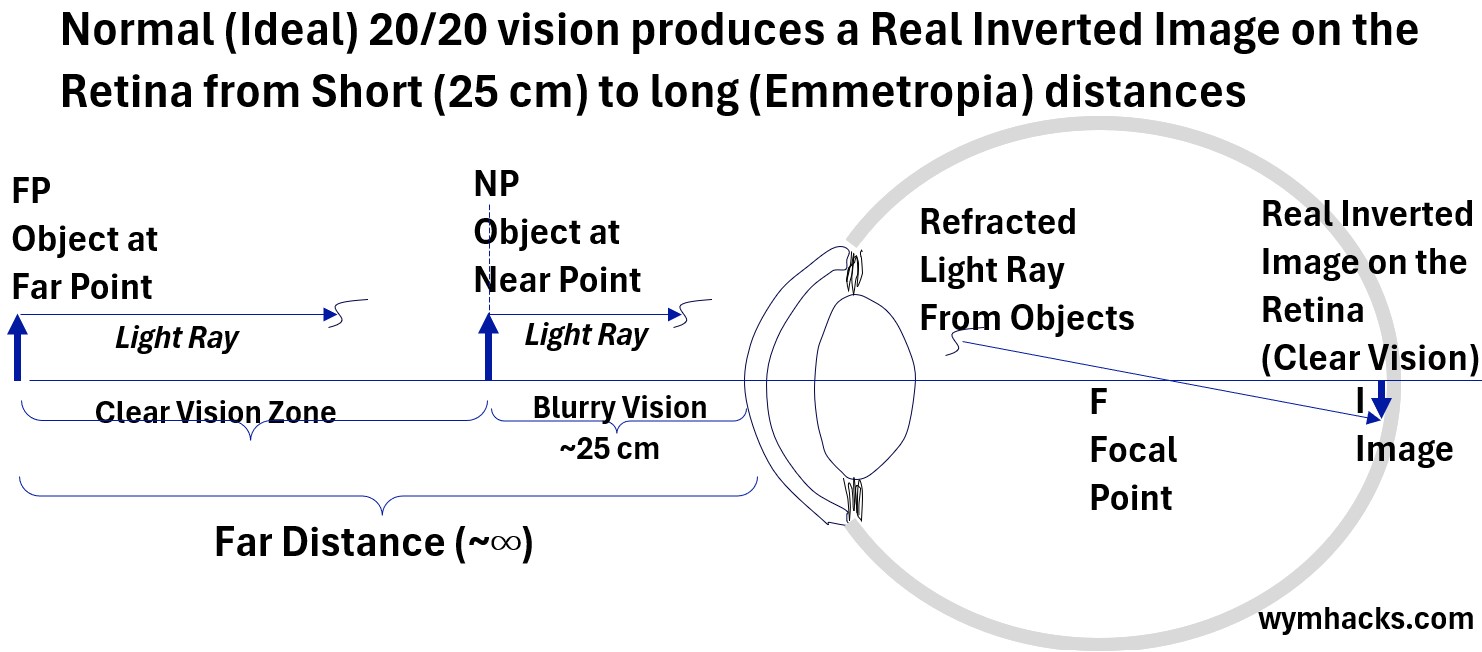
The sketch below shows a simplified ray diagram for a “normal” eye with no refractive errors i.e. the light from an object refracts just right so an inverted image is placed on the Retina at the back of the eyeball.
Picture_Ray Diagram of Normal Eye with No Refractive Errors
If you want to dig more into any of the concepts mentioned above, refer to these posts:
Next, we explore Near and Far Sightedness and the related concepts of Far Point and Near Point.
Near Sightedness and Far Sightedness
Check out the diagram below which compares “normal or perfect vision” to Far and Near Sightedness.
Picture_Near Sightedness and Far Sightedness Defined
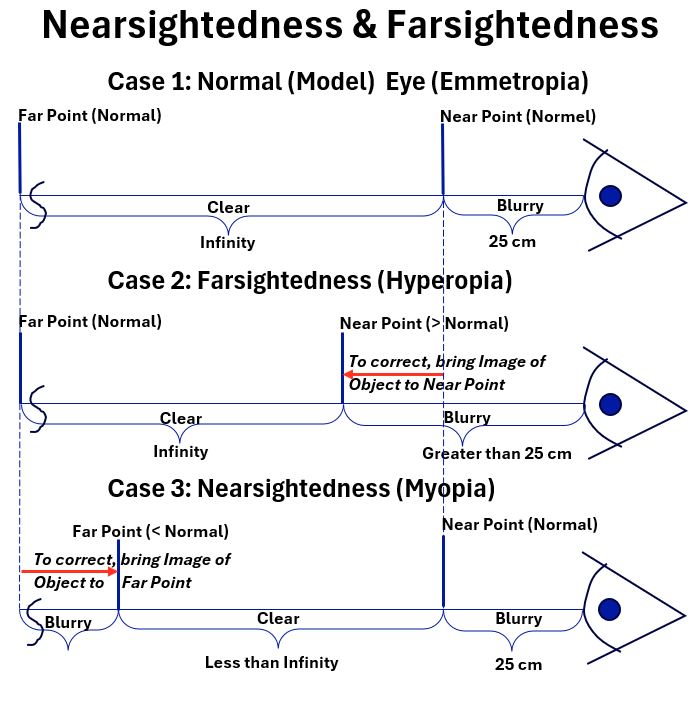
A normal eye, Case 1, doesn’t need vision correction
- The eye sees objects clearly at ~25 centimeters (about 10 inches) or greater.
A Far Sighted eye, Case 2, means short distance vision is not as good as “normal”.
- This typically means that the distance at which close objects can be seen clearly (the Near Point) is greater than 25 cm (10 in).
- Far Sightedness is known as Hyperopia or Hypermetropia
- It affects roughly 10% of the US population.
Structural Causes of Hyperopia
Decreased Axial Length meaning eyeball is shorter than normal from front to back.
Decreased Converging Power of the eye caused by the Cornea (shape), Lens (shape), or eye media.
- Result: Image of an object appears behind the Retina resulting in blurry vision.
- Correction of Far Sightedness brings the image of a close object to the Near Point (increasing distance from eye).
- For example, your Near Point is 100 cm and wearing properly prescribed eye glasses “moves” the image of an object to the Near Point distance so you can see it clearly.
- Correction can be done via glasses, contact lenses, or surgery.
A Near Sighted eye, Case 3, means Long Distance vision is not as good as “normal”
- This means the distance at which far objects can be seen clearly (the Far Point) is less than “normal”.
- Near Sightedness is known as Myopia.
- It affects roughly 20 – 50% of the US population. Most sources indicate numbers on the high side of this range.
Myopia structural causes.
- The eye is longer than normal (increased axial length) (oval shape)
- The Cornea and or Lens are steeper (fatter; thicker in the middle) than normal.
- Result: Optical power of the eye is too strong for the corresponding axial length.
- Result: Object Image is converged too strongly and focuses in front of the Retina resulting in blurry vision.
- Correction of Near Sightedness involves bringing the image of a far object to the Far Point (decreasing distance to the eye)
- Correction can be done via glasses, contact lenses, or surgery.
A Normal Eye With “Perfect” Vision
A normal eye has clear vision of objects located roughly 25 cm (10 inches) or greater from the eye.
The structures of the eye (Cornea and Lens mainly) refract and converge object light rays such that the Focal Point is located close enough to the Retina such that the Object Image falls directly on the Retina.
Note that many simplified drawings don’t reflect this accurately i.e. it’s the Object Image that falls on the Retina and not the Focal Point.
The Image of an Object always projects in the eye as an inverted Real Image.
The brain flips this image and converts it to sight.
Picture_Normal Eye – Clear Vision at 25 (10 inches) cm and further
Near Sightedness, Far Sightedness, Astigmatism, and Presbyopia cause the Object Image to not fall directly on the Retina.
With Farsightedness, the Near Point, the closest distance at which objects can be seen clearly, is greater than “normal”.
With Nearsightedness, the Far Point, the furthest distance at which objects can be seen clearly, is less than “normal”.
Far Sightedness and Its Correction
- the Near Point of the eye is therefore greater than “normal” (> ~ 25 cm)
- your eyeball is shorter than normal and/or
- your Cornea is curved too little (i.e. too steep)
- your lens is curved too little (i.e. too steep)
An insufficiently curved Cornea or Lens weakens its ability to bend light rays (i.e. has less Power).
- The degree of light bending is directly related to the curvature of the surface.
- Power = 1/focal length; See my article Refractive Geometric Optics
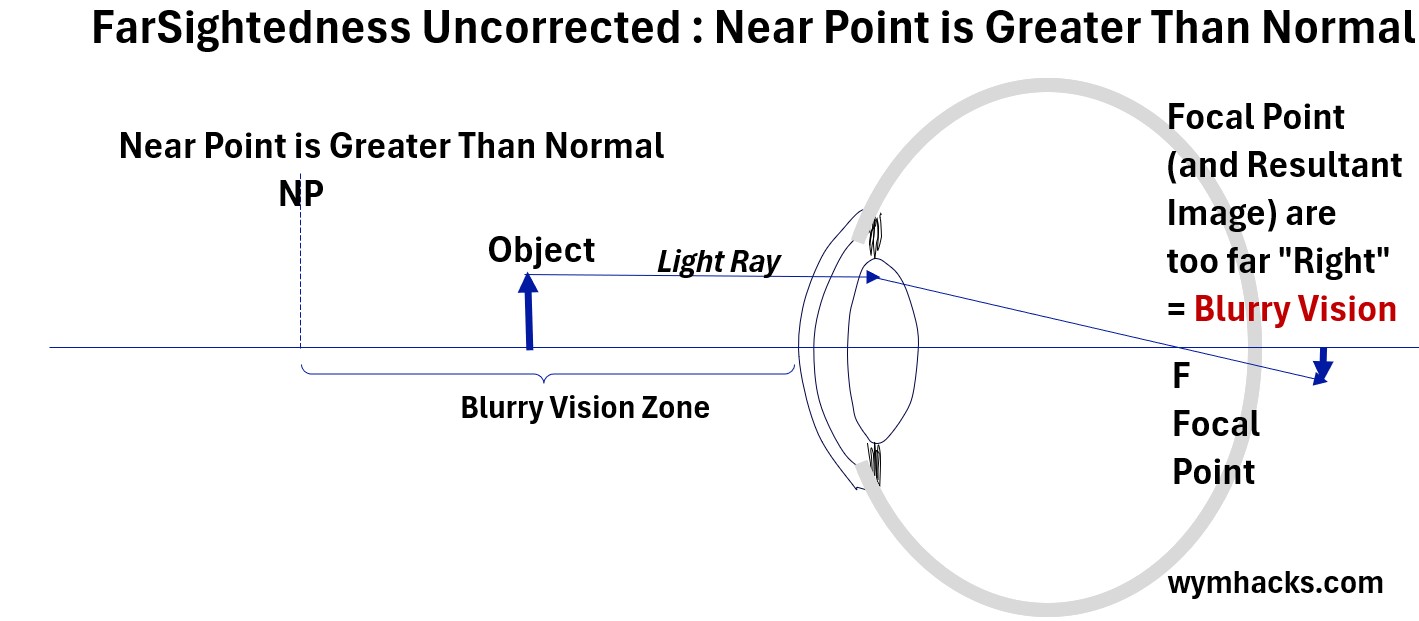
In the picture below, an uncorrected Far Sighted eye focuses too far “to the right”, such that the
- Focal Point is too far right and
- The Object Image is projected too far right, posterior to the Retina
Picture_Farsightedness Uncorrected (Near Point > Normal)
Wearing converging (convex or “plus”) lens eye glasses (or contacts), typically correct Far Sightedness. (see the picture below)
Picture_Farsightedness Corrected: Shift Image Left to Near Point
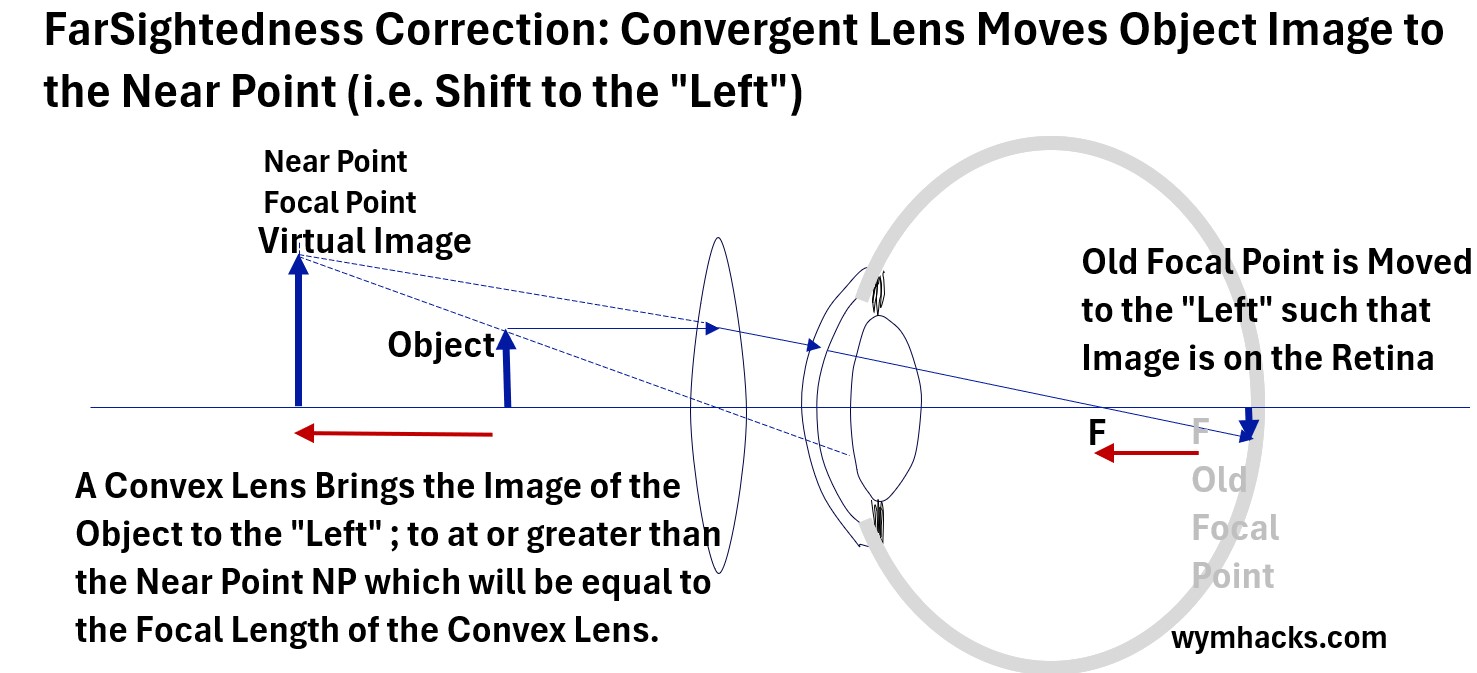
Putting a correctly designed converging lens (convex or “plus” lens) in front of the eye,
- bends light inwards (converges light) towards the eye
- creates a Virtual Image of the near Object at the Near Point of the eye
- where the Near Point is greater than a normal eye Near Point (~25 cm)
- shifts or moves the Focal Point F to the “left” (away from the Retina)
- which shifts the Object Image to the “left” and onto the Retina
It is always true that converging corrective lenses
- correct for Far Sightedness by refracting and converging light inwards towards the eye.
- create a Virtual Image further away from the eye than the Object and at the Near Point.
For converging corrective lenses it’s also always true that the Object is closer to the lens than the Focal Point (the only case in which a virtual image is formed with a convex lens). See my article Refractive Geometric Optics.
It is also always true that the structures of the eye (shape, Cornea, Lens, other media in the eye) refract light inwards (converge towards the central axis of the eye).
- Refer to my post Refractive Geometric Optics for more background on refraction, lens types, ray diagrams and more.
- Refer Michel van Biezen Physics Videos Using Thin Lens Equation
- See the “Physics – Optics: Vision Correction..” video series (1, 4 and 5)
Presbyopia (Loss of Accommodation)
See my post: Eye Lens Anatomy for more on the structure and operation of the lens of the eye.
The picture below shows Anterior and Side views of an eye lens.
In a process called Accommodation, the Ciliary Body and associated ligaments adjust the thickness of the lens to assist the eye in focusing on near or far objects.
Picture_Lens Accommodation (Anterior and Side Views)
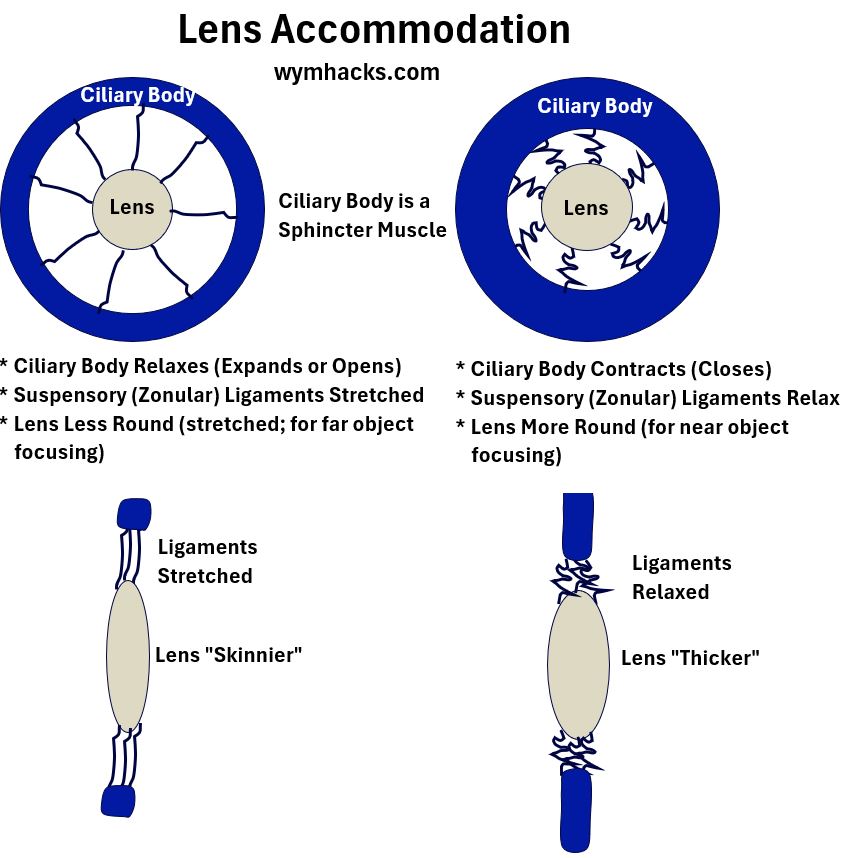
When the Ciliary Body relaxes, it expands or opens, stretches the ligaments, and stretches the Lens
- A stretched, skinner lens allows for far object vision (less power)
- Often models of the eye are provided based on the eye being in a “relaxed condition“.
- This specifically means the Ciliary Bodies are in a relaxed state (i.e. The eye lens is at its maximum length)
When the Ciliary Body contracts, it relaxes the ligaments and causes the lens to become thicker
- A fatter, thicker lens allows for close object vision (more power)
As we age, the lens age and become more rigid.
- In an eventually universal eye condition called Presbyopia, the lens loses its flexibility and becomes less able to change shape to accommodate for different distances.
- This mainly results in difficulty focusing on nearby objects.
- Presbyopia eventually happens to everyone as they age and can be corrected via eyeglasses, contact lenses, surgeries or Eye drops.
- The typical symptoms for Presbyopia will be similar to Far Sightedness (i.e. loss of ability to see close objects clearly. )
Near Sightedness and its Correction
- the Far Point of the eye is therefore less than “normal” (for calculational purposes, normal distance is infinite)
- your eyeball is longer than normal and/or
- your Cornea curves too steeply and/or
- your lens curves too steeply
An overly curved Cornea or Lens over focuses and puts the image to the “left” of the Retina.
- The degree of light bending is directly related to the curvature of the surface.
- Power = 1/focal length; See my article Refractive Geometric Optics
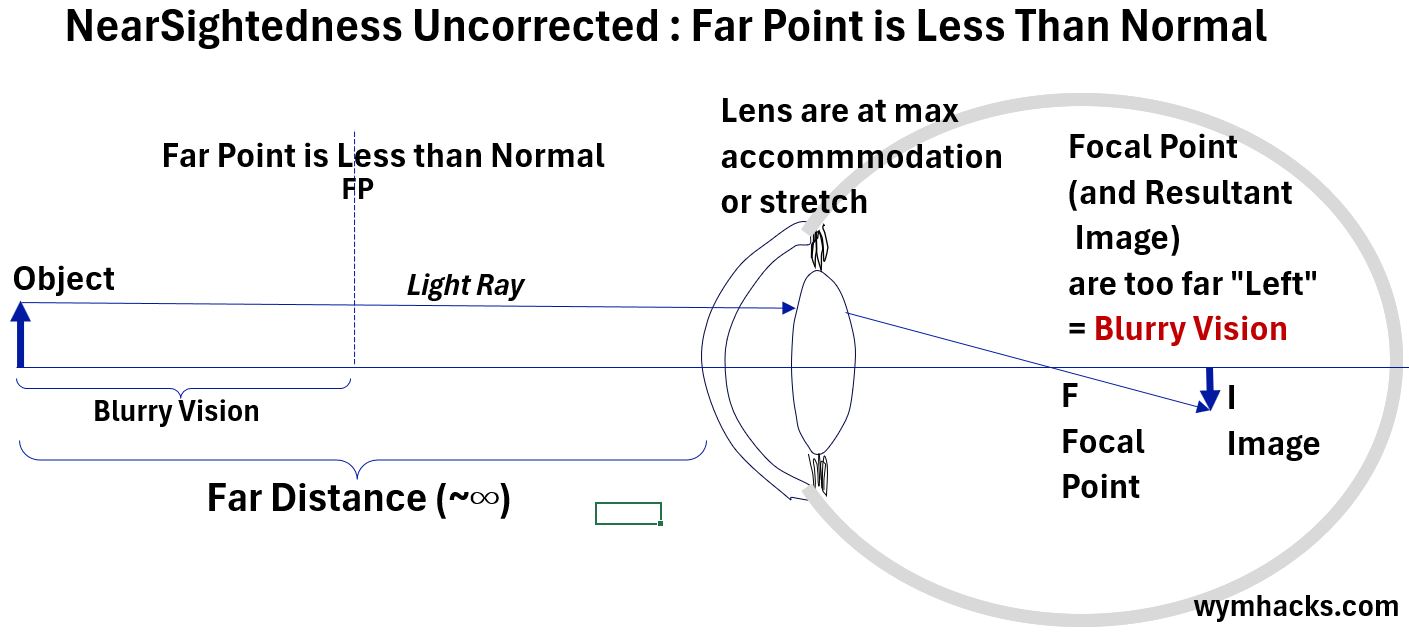
In the picture below, an uncorrected Near Sighted eye focuses too near “to the left”, such that the
- Focal Point is too far left and
- The Object Image is projected too far left, anterior to the Retina
Wearing diverging (concave or “minus”) lens eye glasses (or contacts), typically correct Far Sightedness (see the picture below).
The Object light rays are effectively diverged outwards, before the eye structures converge them inwards. This pushes the Focal Point towards the Retina.
Picture_Nearsightedness Corrected: Shift Image Right to Far Point
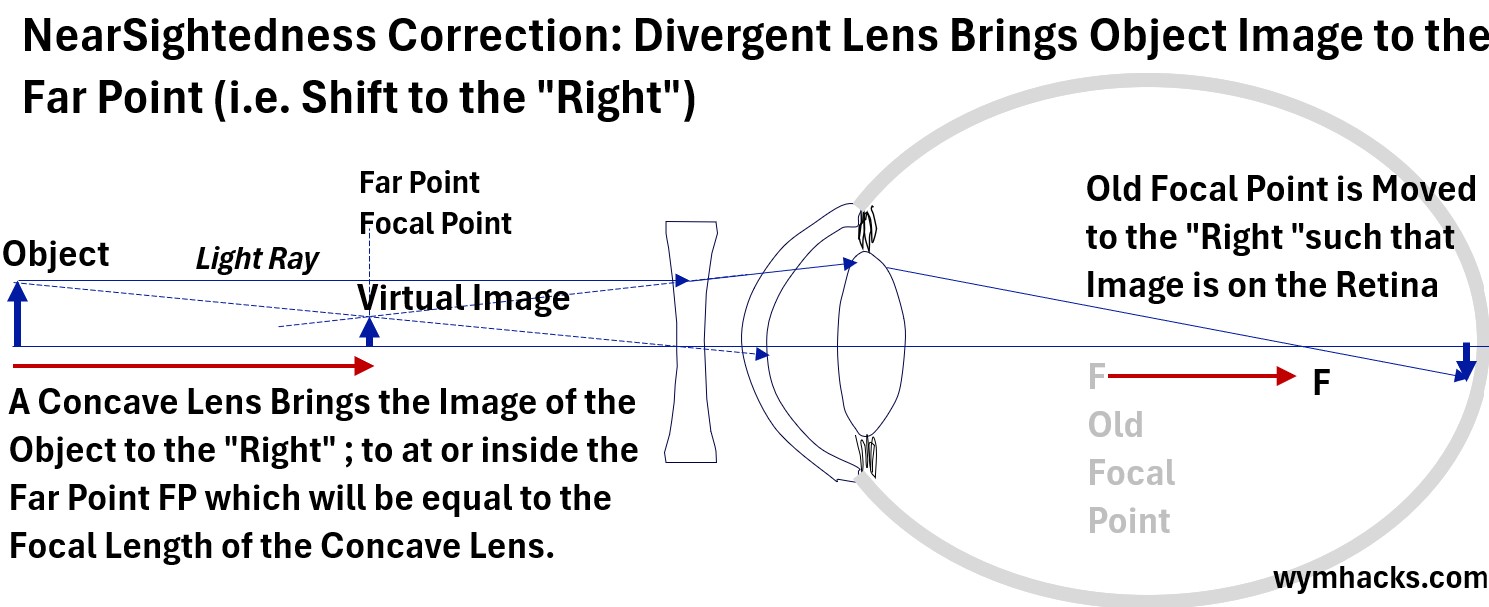
Putting a correctly designed diverging lens (concave or “minus” lens) in front of the eye,
- bends light outwards (diverges light) towards the eye (before the eye converges it back inward)
- creates a Virtual Image of the far Object at the Far Point of the eye
- where the Far Point is less than a normal eye Far Point
- shifts or moves the Focal Point F to the “right” (towards the Retina)
- which shifts the Image to the “right” and onto the Retina
It is always true that diverging corrective lenses
- correct for Near Sightedness by diverging light outwards and towards the eye before the eye converges the light back inward.
- create a Virtual Image closer to the eye than the Object and at the Far Point.
For a diverging corrective lens, the actual object can be located anywhere relative to the focal point of the concave lens. The lens’s job is to create a virtual image that is closer to the eye, regardless of the object’s initial distance. See my article Refractive Geometric Optics.
It is also always true that the structures of the eye (shape, Cornea, Lens, other media in the eye) refract light inwards (converge light towards the central axis of the eye).
- Refer to my post Refractive Geometric Optics for more background on refraction, lens types, ray diagrams and more.
- Refer Michel van Biezen Physics Videos Using Thin Lens Equation
- See the “Physics – Optics: Vision Correction..” video series (1, 2 and 3)
Astigmatism
Astigmatic eyes have Corneas with uneven curvature/s (or, less commonly, the lens…called Lenticular Astigmatism).
Whereas a spherical Cornea will tend to focus light onto a single point, an oval shaped (like an egg or an American football) Cornea, for example, will focus a point source of light onto multiple Focal Lines.
The multiple Focal Lines cause blurry vision, poor eyesight at night, eye strain, etc.
There are some fascinating optics behind Astigmatism.
I can’t cover all the details in this post , but here are some excellent references if you want to drill down.
- 2-4 Introduction to Cylindrical Lenses
- The Conoid of Sturm; Pooja Parthasarathi; Thomas J. Stokkermans; 2023.
- AAO.ORG Chapter 10 Astigmatic Refractive Error – Introduction
- AAO.ORG Chapter 11 Astigmatic Refractive Error – The Conoid of Sturm
- AAO.ORG Chapter 12 Astigmatic Refractive Correction-Retinoscopy Basic Optics
- AAO.ORG Chapter 13 Astigmatic Refractive Correction-Jackson Cross
- AAO.ORG Chapter 14 Astigmatic Refractive Error – Types of Astigmatism
- AAO.ORG Chapter 15 Astigmatic Refractive Error: The Power Cross
Focal Lines
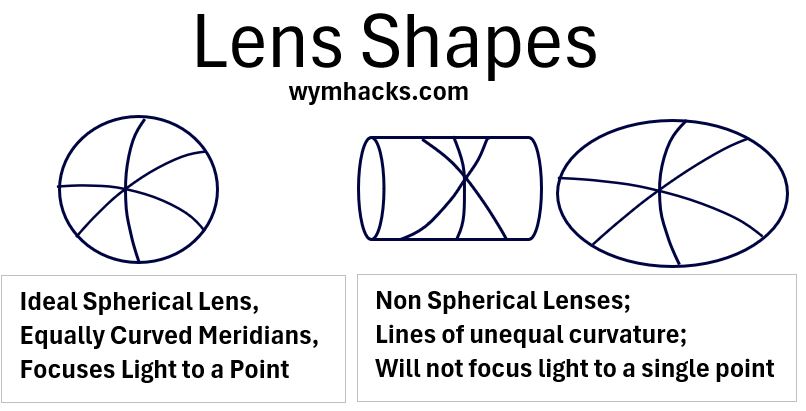
Parallel light rays from a point source entering a non spherical lens (elliptical or cylindrical for example) will form Focal Lines and not a point.
- Read the Chapter 10 and 11 links provided above to learn more about this.
Picture_Only a Spherical Lens Will have Lines of Equal Length and Curvature
There are two general types of Astigmatism, Irregular Astigmatism and Regular Astigmatism.
Regular Astigmatism
In Regular Astigmatism,
- the refractive power (P = 1/f) of the eye (the lens) changes uniformly and proportionally from one meridian (line of curvature) to the next.
- the axes of the Principal Meridians (the meridians whose curvatures differ the most) are perpendicular to one another.
Note, that each line of curvature produces its Focal lines, but focusing on the maximum and minimum cases, allows for optimal correction.
Irregular Astigmatism
In Irregular Astigmatism, the
- Refractive Power of a lens does not change smoothly and proportionally from one line of curvature (meridian) to the next.
- two principal meridians may not be orthogonal (perpendicular) and cannot be corrected with glasses.
- an irregular Corneal surface
- Postoperative causes (e.g. after eye surgery)
- Lens issues (e.g. cataracts, others)
Regular Astigmatism – Orientation
For Regularly Astigmatic eyes, the shape of the Cornea departs from a roughly spherical shape and typically assumes an oval or egg shape as shown in the pictures below.
WTR (With-the-Rule) and ATR (Against-the-Rule) Astigmatism describe the orientation of the steepest and least steep curves:
- WTR: The steepest curve of the Cornea is oriented vertically.
- ATR: The steepest curve is oriented horizontally.
Picture_Astigmatic Cornea _ With the Rule_Against the Rule
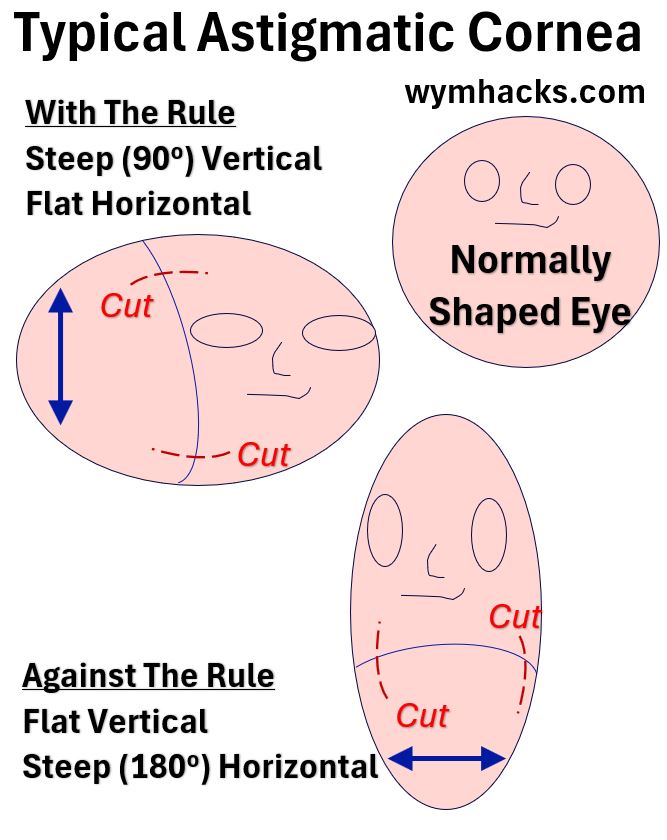
- These are just indicative surgical cut points that an opthamologist might make to cause the shape to change to a more spherical shape (and therefore reduce or remove the Astigmatism).
- This surgical procedure is sometimes called an Arcuate Keratotomy.
- A With the Rule (WTR) plane would be at roughly 90 degrees.
- An Against the Rule (ATR) plane would be located at roughly 180 degrees.
Regular Astigmatism – Focal Point Lines
In the simplified drawing below, the vertical plane of the Cornea has the steepest curvature (With The Rule).
This results in two differently located Focal Lines (1 and 2) , which result in two images focused differently (i.e. Blurry Vision).
Picture_Astigmatism Results in Multiple Focal Points and Blurriness
The vertical steeper plane shown above converges light onto a Focal Point on Line 1.
- Imagine several other vertical planes made to the left and right of the vertical plane in the picture.
- Light is converged by these planes onto other Focal Points located on the same Focal Line 1
- The end result is a Focal Line 1, which is perpendicular to the vertical planes.
The least steep horizontal plane shown above converges light onto a Focal Point on Line 2
- Using the same logic described above, a Focal Line 2 is formed and is perpendicular to the horizontal planes.
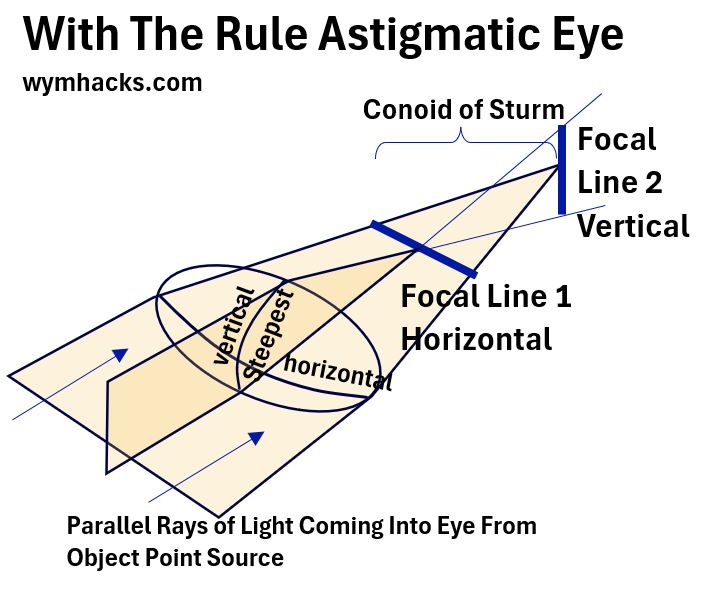
Regular Astigmatism – Conoid of Sturm
In the Conoid of Sturm, the space between the Focal Lines 1 and 2, various shapes of light appear.
Picture_Conoid of Sturm_With The Rule Eye
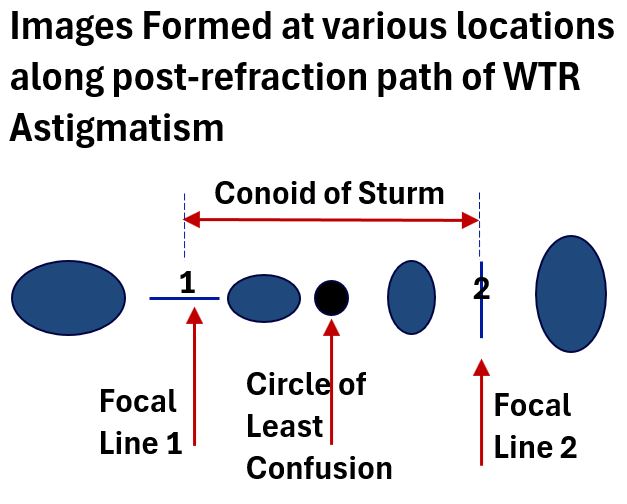
The Circle of Least Confusion, you’ve got to love that name, is the least blurry image located between the Focal Lines.
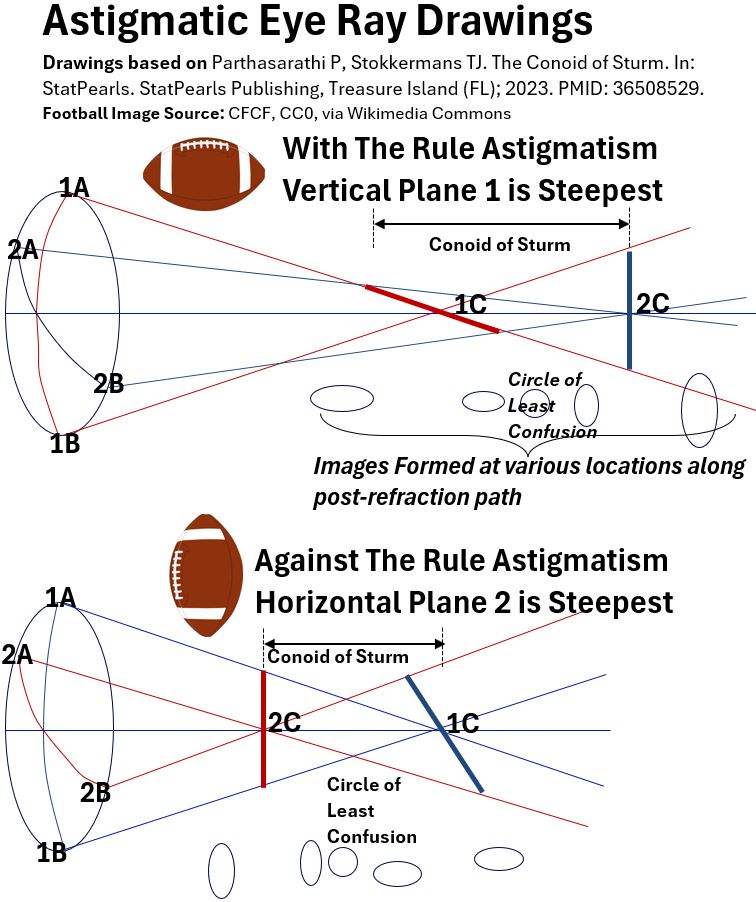
Just for completeness, in the drawing below, I’ve drawn indicative Astigmatic eye Ray Drawings for With The Rule and Against The Rule Astigmatic eyes.
- The drawings are based on this nice article: The Conoid of Sturm by Parthasarathi P and Stokkermans TJ ; 2022.
Picture_WTR and ATR Astigmatic Eye Ray Drawings
Regular Astigmatism – Just Two Focal Lines Being Produced?
You might be asking yourself, well,
- what about all the other meridians in an Astigmatic eye?
- Dont each of them make a different Focal Line? That is,
- don’t we really have a continuum of Focal Lines produced by each curved plane of an Astigmatic eye?
I think the answer is yes, but
- in a Regular Astigmatic eye, the steepest and least steep refractive planes (curves) are identified.
- These represent the extremes in differences in focus.
- We only need to focus on these to optimize a vision correction.
- That is, correcting these extreme ranges should effectively correct all other differences in between.
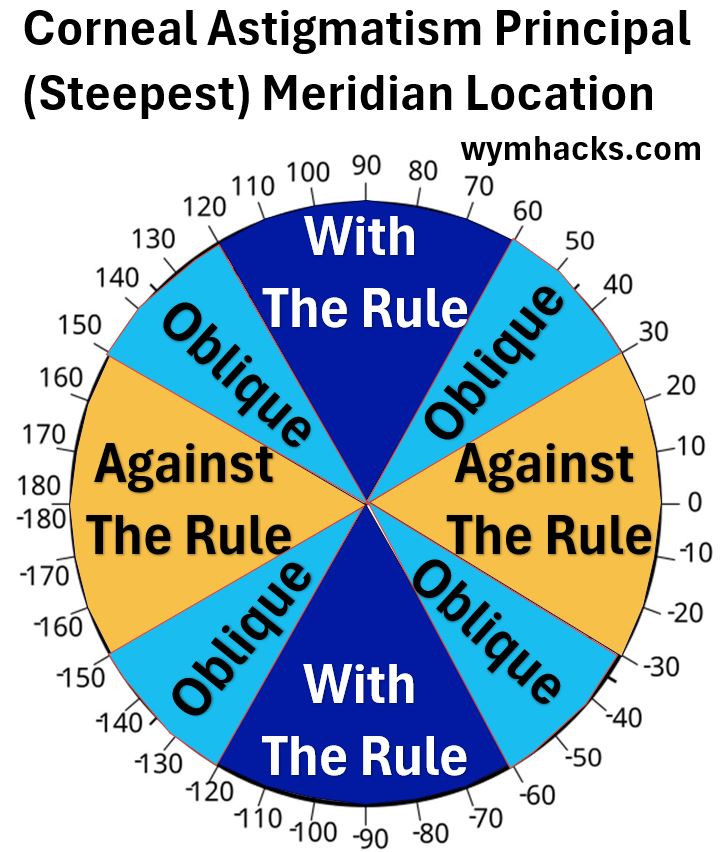
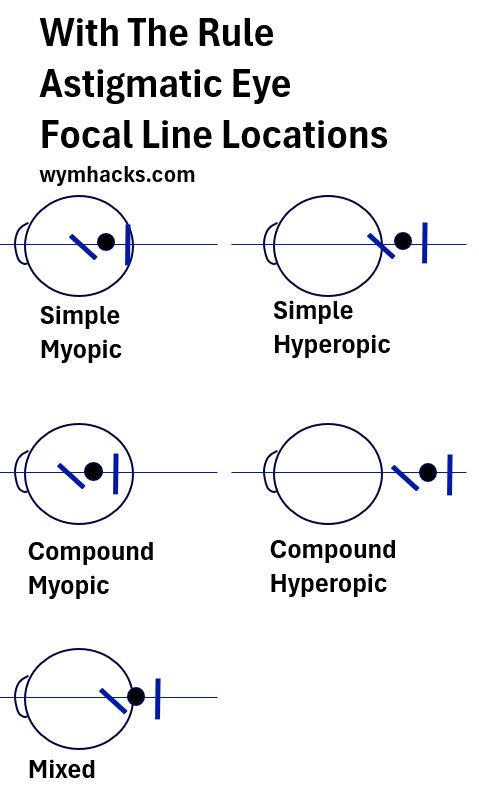
Regular Astigmatism – Location of Focal Point Lines
Picture_Conoid of Sturm Locations for With The Rule Astigmatism
Astigmatism Correction – Glasses or Contact (Toric) Lenses
In order to correct for any refractive error, we want to place a focused image onto the back of the Retina at the Fovea.
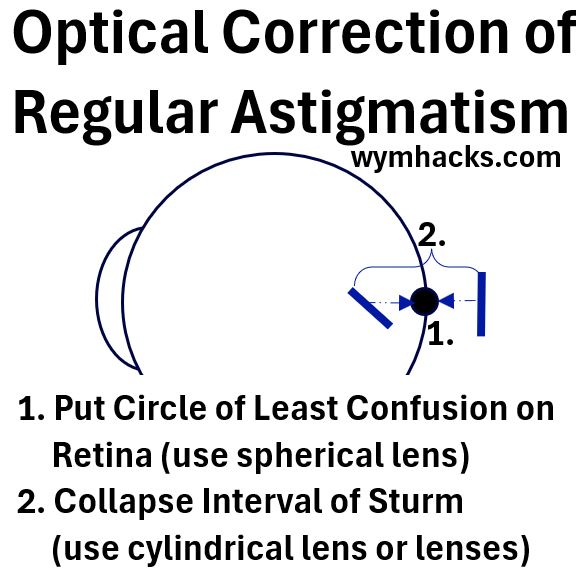
Two “things’ have to happen in order to correct Astigmatism using glasses or “toric” contact lenses.
1) The Circle of Least Confusion needs to be located on the Retina.
- This results in the least distorted picture
- A spherical lens does this.
But to get the optimal correction we also have to
2) Collapse the Interval of Sturm
- This improves on 1.
- A cylindrical lens (or lenses) collapses the conoid of Sturm onto the Retina and
- the pair of Focal Lines reduce to a single Focal Point.
Astigmatism Correction
Glasses and contact lenses can correct Astigmatism.
Surgical procedures like LASIK and PRK and others (e.g. Limbal Relaxing Incisions) will also correct Astigmatism.
Next, let’s take a closer look at some of the common tools and procedures that correct Refractive Errors.
Eyeglass/Contact Prescription
Table – Glasses Prescription Details
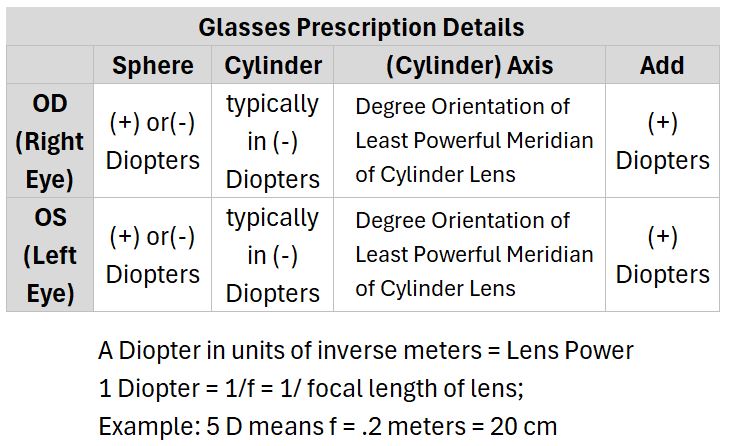
- OD is short for the Latin “Oculus Dexter” or right eye
- OS is short for “Oculus Sinister” , Latin for left eye
- The English word Sinister meaning bad or evil comes from the same Latin word for Left (as in Left handed).
- Here is an interesting article on how this came to be
- The Spherical lens is the most basic kind of lens used for vision correction (the convex and concave ones we’ve described in this post)
- The bigger the number, the higher the power.
- The units are Diopters. A Diopter is equal to the reciprocal of the focal length of the lens.
- (+) values correct for Far Sightedness and (-) values correct for Near Sightedness
- See my post Refractive Geometric Optics for more on Diopters, Focal Length, and the thin lens equation
- Refer Michel van Biezen Physics Videos Using Thin Lens Equation
- See the “Physics – Optics: Vision Correction..” video series (1-5)
- The Cylinder Lens is used to correct Astigmatism. I am nearsighted and I have Astigmatism, so my glasses will be a combination of spherical and cylindrical lenses
- There is just a single power provided in Diopter , which is usually presented as a negative value.
- There is a way to convert the negative value to a positive value so you might see it presented this way as well
- The Axis is the orientation that the cylinder has to be placed in relative to your eye for it to correct properly. Its the direction of the minimum (or zero) cylindrical power.
- The Add indicates you have some kind of reading glass capability in your glasses (maybe bifocal or “progressive” lenses).
- The Add is always a positive value meaning it is magnifying.
Return to Menu
Refractive Vision Error Corrective Procedures
The table below lists some of the vision correction solutions for Refractive Errors.
Table_Vision Correction Procedures
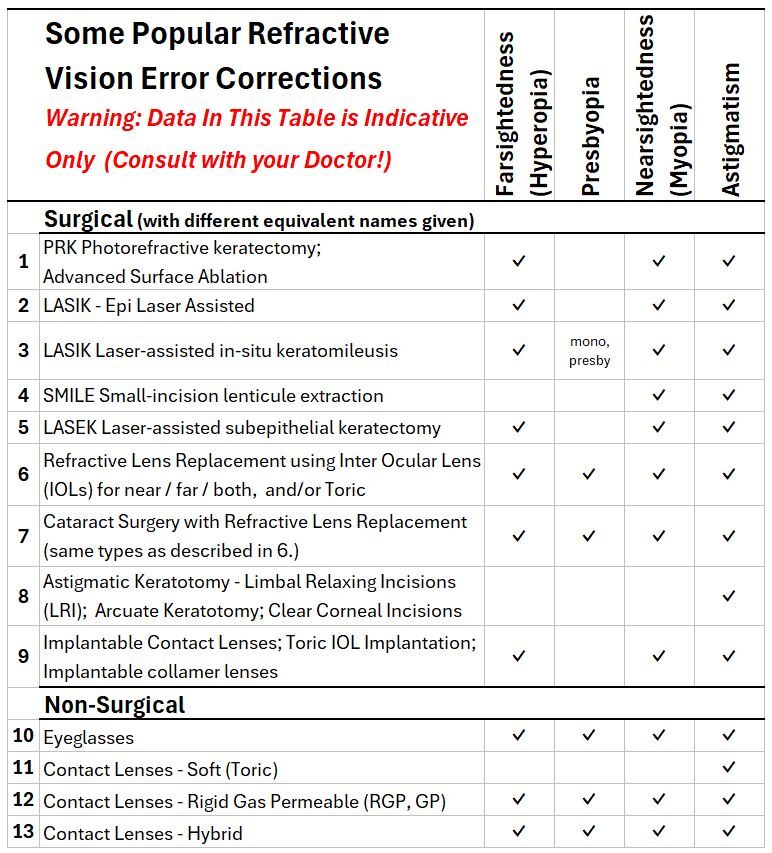
Note: A person can have both Near Sightedness and Far Sightedness but not in the same eyeball.
Many will be able to correct all their refractive errors with eye glasses or contacts.
But sometimes, you might be forced to do something surgically like
- when your eye lenses start to become opaque (cataracts) or you have some other eye condition.
- Or you might just want to ditch the glasses you’ve had to wear on your face since you were 5.
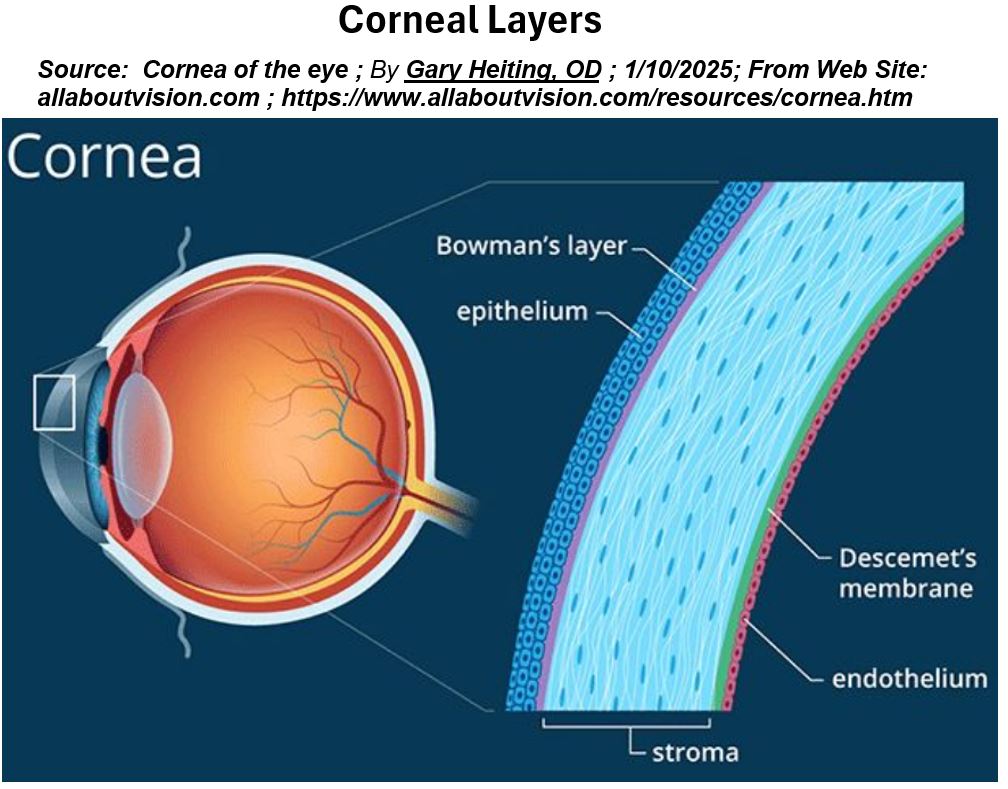
I describe some of the surgical options below but first familiarize yourself with the picture below showing the layers of the Cornea.
All Corneal reshaping surgical procedures will impact the top three layers: Epithelium, Bowman’s Layer, and the Stroma.
See the Cornea section in my post Eye Anatomy for more information on what these layers do.
Picture_Corneal Layers
PRK Photorefractive keratectomy
- Corrects Myopia, Hyperopia, and Astigmatism.
- A first generation process employing “surface” treatment.
- PRK Treatment Animation
- Step 1: Top surface Epithelium (gently!) scraped away.
- Step 2: A computer-controlled excimer laser reshapes (ablates) the Stroma
- Cover healing eye with temporary contact lens till Epithelium grows back in.
LASIK Laser-assisted in-situ keratomileusis
- Corrects Myopia, Hyperopia, and Astigmatism.
- A second generation procedure.
- LASIK Treatment Animation
- Step 1: Cut a A thin flap (~130 to 180 microns thick) using one kind of laser with a tool called a microkeratome.
- Step 2: Another laser reshapes the Stromal tissue (excimer laser ablation)
flap is repositioned and edges of flap heal
LASEK Laser-assisted subepithelial keratectomy
- A hybrid of PRK and LASIK where the Epithelium is preserved.
- LASEK Animation
- Step 1: Treat Epithelium with alcohol, loosen and separate it from the Stroma, and roll it back.
- Step 2: an excimer laser ablates the underlying Stroma and the Epithelial cells are rolled back out.
- Possible advantages of LASEK are to speed recovery and reduce pain
LASIK – Epi Laser Assisted In Situ Keratomileusis
- Also a surface treatment process.
- An improvement on the PRK procedure.
- New (relatively speaking) procedure designed to avoid risks and reduce pain associated with LASIK or PRK.
- With an Epi Laser, a very thin Epithelial sheet is moved to the side.
- After Corneal reshaping, the thin Epithelial sheet can be rolled back on or removed.
SMILE Small-incision lenticule extraction
- A third generation procedure (PRK and LASIK being first and second)
- SMILE with Femtosecond Laser
- FDA approved for Nearsightedness and Astigmatism correction.
- Performed using a femtosecond laser.
- Step 1: The laser carves out a small lens-shaped bit of tissue (lenticule) within the Cornea.
- Step 2: The same laser cuts a small arc-shaped incision in the surface of the Cornea and the surgeon extracts the lenticule.
Removing the tiny lenticule changes the shape of the Cornea and corrects Nearsightedness and Astigmatism.
Phakic IOLs: Implantable Lenses
- Correct for Nearsightedness.
- Phakic intraocular lenses, or phakic lenses, are lenses that are implanted into the eye permanently.
- Phakic comes from the Greek Phakos which means “lens.
- Function like contact lenses but they are inside the eye.
- The lens is implanted into the eye without removing the eye’s natural lens.
- Natural lens accommodation still functional
Intraocular Lens (IOL) Implants
The natural lens of the eyes can be replaced due to cataracts and/or other reasons.
The term Refractive Lens Exchange (RLE) or Replacement is a broad term indicating the replacement of lens for any number of reasons.
This would include removing lens primarily because they are cloudy from cataracts.
- For an excellent animation of both a traditional and laser assisted cataract surgery,
The term Clear Lens Exchange (CLE) specifically means removing a clear, non-cataract-affected lens.
- A CLE could correct Nearsightedness (myopia), Farsightedness (hyperopia), Presbyopia , and/or Astigmatism.
- Recommended for people in their mid- or late-50s or slightly younger people who need reading glasses.
- This solves the issue of having cataracts in the future as well.
- IOLs that can correct Astigmatism are called toric IOLs.
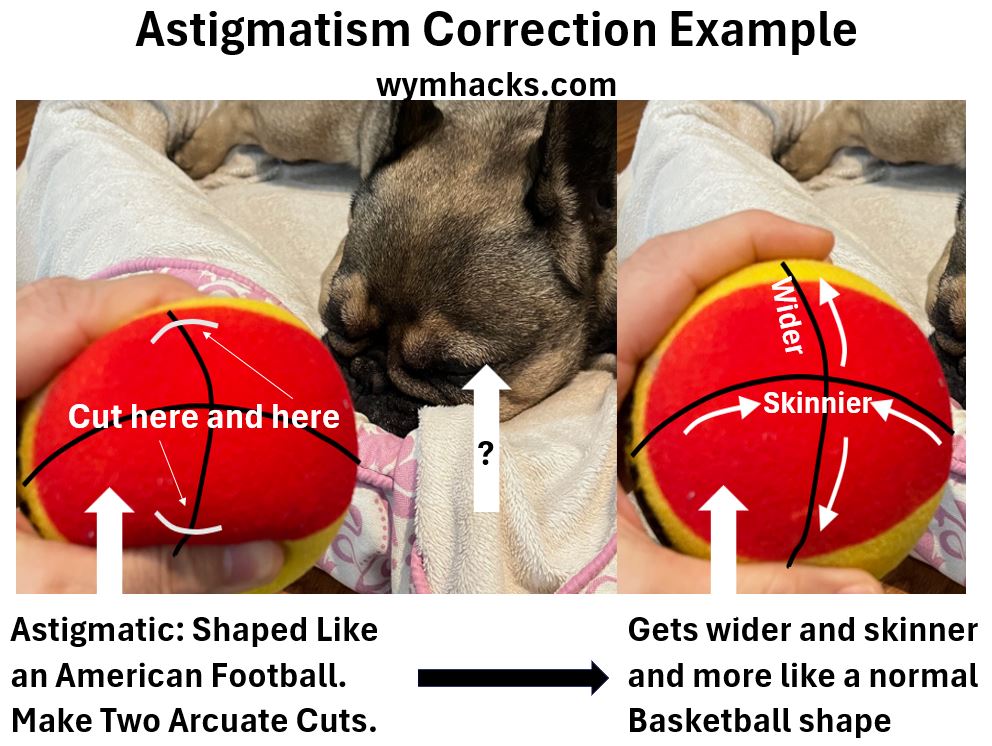
Incisions on the Cornea to Correct Astigmatism
- Astigmatism can be treated by making small incisions on the Cornea
- I had this done to my eyes during my cataract surgery (same laser instrument was used).
- The incisions, made perpendicular to the steepest plane will “flatten” the Cornea (make it more spherical).
- In the picture below, the ball represents the Cornea.
- This illustrates a “With The Rule Astigmatic Cornea” (an oblate Cornea).
- Perpendicular cuts in the steeper vertical plane will make the ball more “round” again.

- Corneal incisions for Astigmatism are called
- Limbal Relaxing Incisions (LRIs) – more peripheral cuts,
- Astigmatic Keratotomy (AK) – less peripheral cuts
- Arcuate Keratotomy (also AK).
- Clear Corneal Incisions
- Watch this awesome detailed tutorial on Limbal Relaxing Incisions by Uday Devgan
- Look at the diagrams at 09/5:49 (Coupling Effect) ;1:33/5:49 (Larger Incisions), 2:51/5:49 (Central Incisions) and 3:50/5:49 (Deeper Incisions)