
(DGA) Dietary Guidelines for Americans
These guidelines are revised/reviewed/updated every 5 years. You can find the latest documents here:
Before I display the tabulated values, let’s first get clear on a few definitions.
Definitions
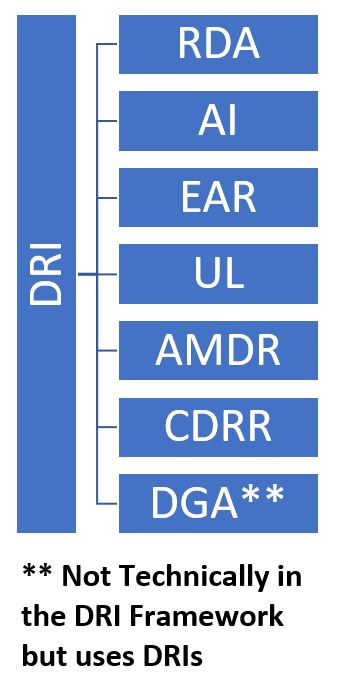
The DGA guidelines are (mostly) based on Dietary Reference Intakes (DRIs)
- The DRIs (Dietary Reference Intakes) are the foundation
- They are a comprehensive set of science-based reference values for nutrients.
- The DRIs provide values under various sub-descriptors (e.g. RDA and others).
- AMDR, RDA, EAR, UL, AI, and CDRR are specific terms within the DRI framework – each addressing different aspects of nutrient needs.
- The DGA (Dietary Guidelines for Americans) builds upon the DRIs.
- The DGA uses the scientific basis provided by DRIs to create practical dietary recommendations for the US population.
- So, the DRIs act as the scientific backbone, informing both the specific nutrient reference values within the system and broader dietary guidance like the DGA.
For more on the DRIs and the specific definitions of the various sub-terms refer to:
Meaning of the Recommended Values
The values in the DGA table(s) below indicate adequate levels of the specific nutrient, and, on any particular day, you should be roughly taking in the amounts indicated in the tables.
Please note though, that there is a level of “conservativeness” built into the values.
For example, the RDA (Recommended Dietary Allowance) is the average amount in a healthy population + 2 Standard Deviations.
In statistics, for a normally distributed sampling of data, including 2 standard deviations means about 95% of the data falls within this value.
For example, the Estimated Average Requirement (EAR; the average) for protein for adults is .66 g/kg weight while the RDA (the average + at least 2 standard deviations) for protein for adults is .8 g/kg.
You’ll often hear the term insufficient vs deficient.
- Nutrient Insufficiency is the state where a nutrient intake amount is below the guideline for your age and sex.
- So, a long term insufficiency can increase the risk of developing a deficiency over time.
- A Nutrient Deficiency is a more severe state (than insufficiency) where your body lacks sufficient amounts of a specific nutrient to function properly.
- A deficiency would be expected to lead to deleterious body symptoms.
Dietary Guidelines for Americans Chart
Reference Sources:
- https://www.dietaryguidelines.gov/ ;
- Table A1-2:Daily Nutritional Goals, Ages 2 and Older; Page 133
- Dietary Guidelines for Americans, 2020-2025 | Appendix 1
- Go to Appendix 2 if you want to understand more about the Source terms (see the “Source a” column in the tables below).
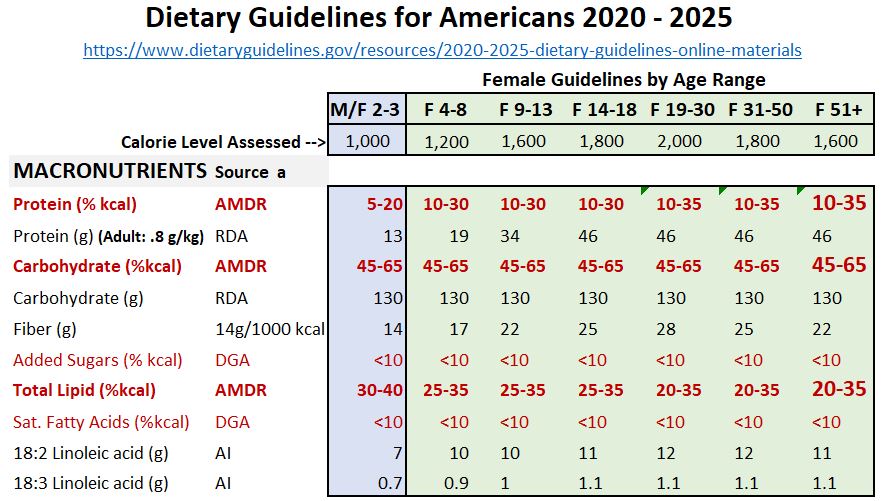
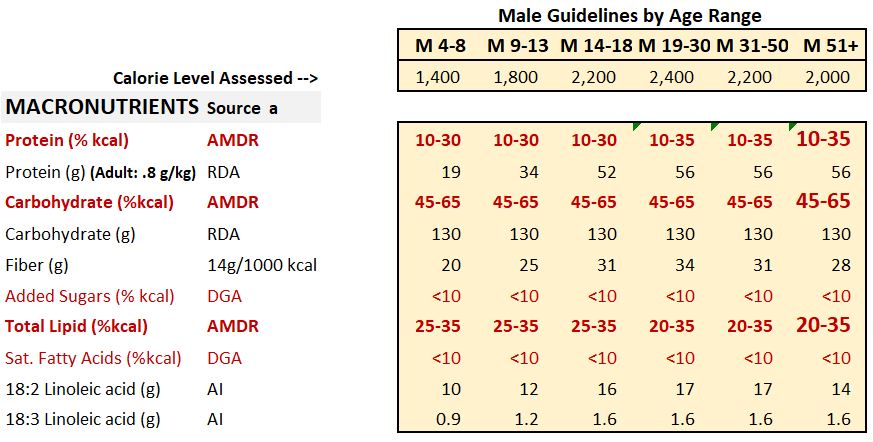
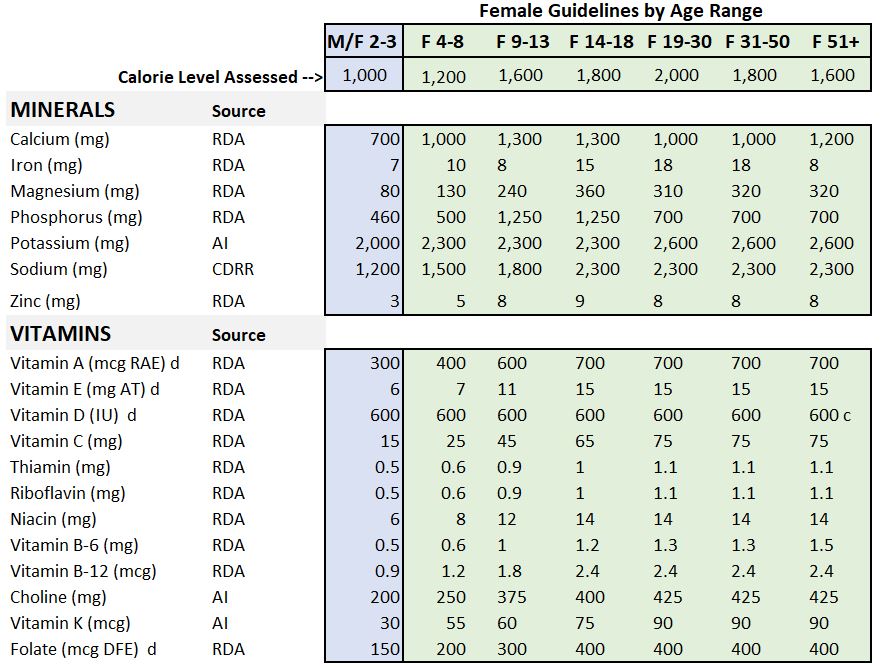
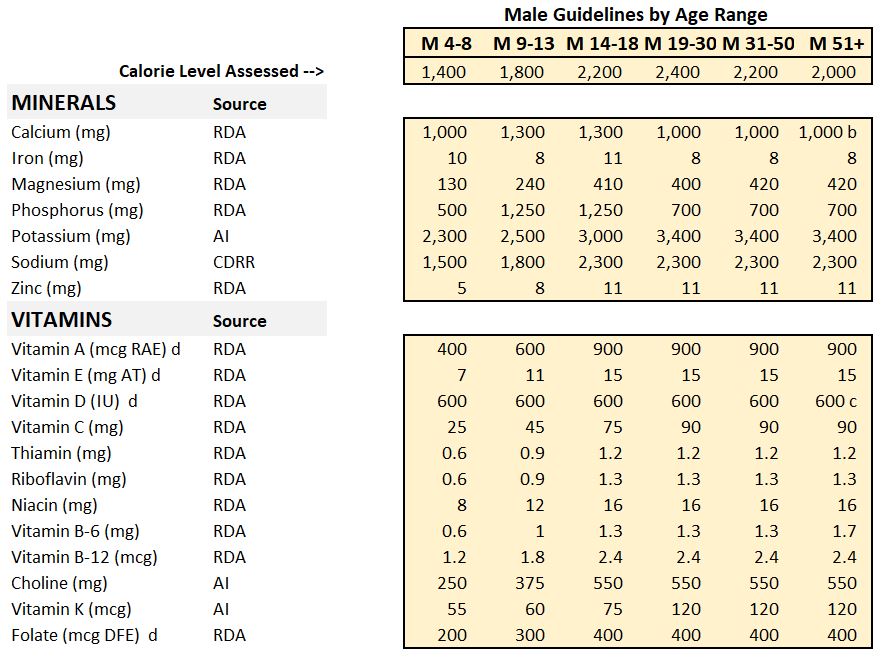
Table Notes
- I provide additional details for:
- AI = Adequate Intake
- RDA = Recommended Dietary Allowance
- CDRR = Chronic Disease Risk Reduction Level
- g = grams (there are about 453.6 grams in a pound or lb)
- mg = milligrams = 1e-3 grams = 1 thousandth (1/1,000) of a gram
- mcg = microgram = 1e-6 grams = 1 millionth (1/1,000,000) of a gram
- IU = International Unit = Specific for each nutrient
- Refer to Appendix 2 for more information on the terms and the units of measure
- For example, the term IU, International Units, is defined differently for different nutrients.
Americans Underperform Nutritionally
, but the chart below says it all.
Based on the DGA guidelines, Americans are woefully deficient in their intakes of most food groups.
Chart – Dietary Intakes Compared to Recommendations
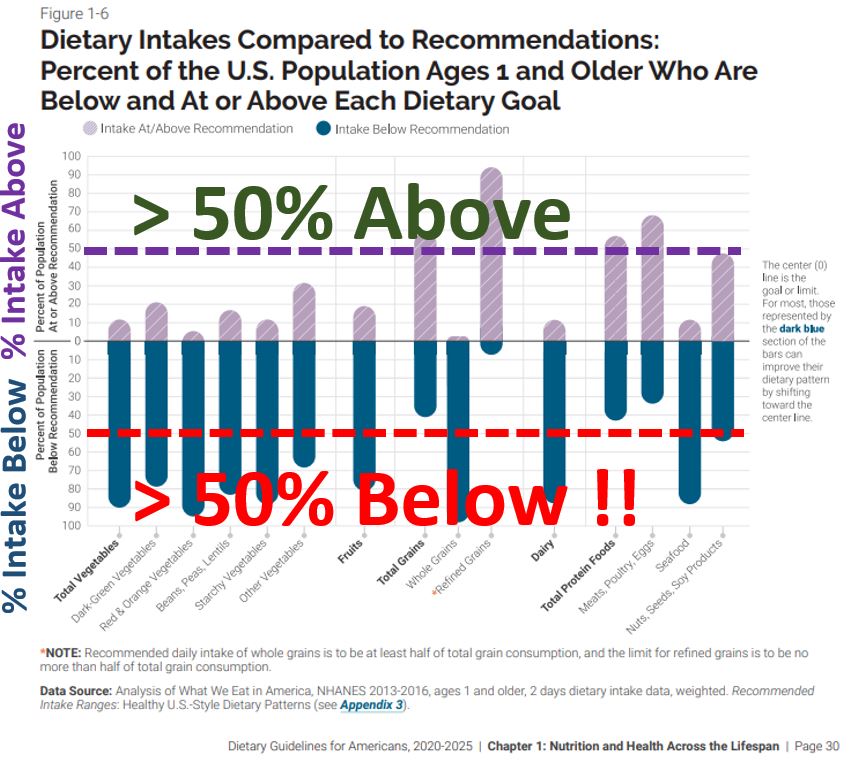
- You are hardly eating enough vegetables and fruits.
- Your grain intakes are heavily weighted towards refined grains.
- Refined grains have less nutrients and are not as healthy as the whole grains.
- Your meat intake is ok except for sea food
- Certain fish are the best source of omega-3 fatty acids which your body and brain need
The sad reality is, fresh healthy food is often more expensive and less accessible than less healthy fast food.
So, I don’t think it’s necessarily an easy thing to meet the DGAs. Its worth trying though.
What is your Status?
- What is your status?
- Are you eating sufficient amounts of the recommended foods?
- Are you getting sufficient amounts of macronutrients, vitamins, and minerals?
- Why not use a free APP like Cronometer or MyFitnessPal ?
- Consider tracking your nutrient intakes to establish your baseline.
- You can then adjust/optimize as needed.
- I take supplements to fill my dietary gaps but,
- I try to maximize the other things first (exercise and nutrients from food)
Even the government recognizes that supplementation to fill nutritional gaps might be necessary.
They provide quite a bit of information and guidance on this topic.
- See the NIH Dietary Supplement Fact Sheets.
Some Studies Don’t Support Supplement Benefit Claims
Be aware that there are large and well regarded studies that have shown no statistical connection between taking multivitamin supplements and reducing the risk of cancer or heart disease:
- For the following study links, keep in mind:
- These studies don’t address other potential health benefits
- e.g. bone health, reducing inflammation, improving mood, improving sleep, etc.
- Results are often based on questionnaires.
- So, the questions themselves could bias the results.
- These studies don’t address other potential health benefits
- JAMA 2024 :Multivitamin Use & Mortality Risk in 3 Prospective US Cohorts
- hopkinsmedicine.org: Is there really any benefit to multivitamins
- 2013: Stop wasting money on vitamin and mineral supplements
My Approach Regarding Nutrient Deficiencies
- I try to exercise regularly.
- I think your body will forgive you for a lot of other bad things you are doing to it if you exercise regularly.
- I Mix in cardio and strength fitness routines. I think we need both.
- I try to consume as well rounded a diet as I can.
- I try to avoid added sugar and minimize alcohol intake.
- I’ve studied my diet and have some roughly estimated nutritional gaps
- I try to adjust my diet as well as take supplements to fill the gaps
- I recognize that I have to try to substantiate any benefit claims that I read or hear about.
- I rely on two main guiding references for nutrition targets and limits:
- the latest DGAs and
- the NIH Dietary Supplement Fact Sheets
Protein
The US RDA (Recommended Dietary Allowance) for Protein (for Adults; 19+) is . 8 grams protein for each kilogram of body weight (.8 g/kg).
- Ranges between 13g/day to 52 g/day for ages less than 19 years).
- The target ratio g/kg varies for younger people (.85 g/kg for ages 4 – 13, 1 g/kg for 14-18 males and .85 for 14-18 females).
- Source: DGA table for RDAs;
- https://www.dietaryguidelines.gov/ ;
- Table A1-2:Daily Nutritional Goals,
- Ages 2 and Older; Page 133 | Dietary Guidelines for Americans, 2020-2025 | Appendix 1; Go to Appendix 2 for detailed definitions. NIH Factsheets Exercise And Athletic Performance
Protein RDA (It’s the average “plus some”)
- The RDA is supposed to be conservative and cover the average plus some more (defined statistically with a value called the standard deviation).
- So the RDA meets the nutrient requirement of nearly all (97 to 98 percent) healthy individuals in a group.
- Statistically you get there (just about) if you add 2 standard deviations to the average.
- The RDA for Protein (for Adults) is .8 g/kg = .66 + 2 Standard Deviations
- Recommended Dietary Allowance (RDA): the average daily dietary intake level that is sufficient to meet the nutrient requirement of nearly all (97 to 98 percent) healthy individuals in a group.
- Technically, 2 standard deviations of a normally distributed set of data represents 95% of the population
- I’m not sure what logic was used to land on 97 to 98%. Regardless, main point is most of the sample population should get an adequate amount at .8 g/kg.
- EAR for Adults for Protein is .66 grams /kg weight
- Estimated Average Requirement (EAR): a nutrient intake value that is estimated to meet the requirement of half the healthy individuals in a group.
- There are no Tolerable Upper Intake Levels (UL) provided for Protein
- Tolerable Upper Intake Level (UL): the highest level of daily nutrient intake that is likely to pose no risk of adverse health effects to almost all individuals in the general population.
- As intake increases above the UL, the risk of adverse effects increases.
Protein Ranges Recommended by Various Experts
- The (.8 g protein)/(kg body weight) RDA for protein is interpreted by some to be the level to stay above to avoid deficiency.
- Many interpret the .8 to be suboptimal for healthspan.
- The exact optimal amount varies depending on the expert but 1.2 g/kg to 1.6 g/kg is often quoted.
- Peter Attia recommends 2 g/kg.
- Higher amounts might be needed for physically active people and for older people (older people can suffer from sarcopenia, a progressive loss of muscle mass).
- Sarcopenia is a common condition that affects most aging adults.
- It is characterized by a gradual loss of muscle mass and strength.
- It can be accelerated by, inactivity, poor nutrition, and chronic diseases.
- I think you should determine your typical protein intake and determine if you at least meet the .8 g/kg RDA.
- In my view, if you are physically active or “old” (I don’t know…lets say over 50) , consider increasing your intake to perhaps 1.2 or 1.6. This hopefully counteracts your body’s natural shedding of muscle.
Leucine and Methionine
The Essential Amino Acids Methionine and Lysine are typically lower in plant-based proteins compared with animal-based proteins.
If you are designing a plant based diet, keep that in mind to ensure you get enough Methionine and Lysine.
According to Google/Gemini,
- “Methionine: This amino acid is important for protein synthesis, tissue repair, and detoxification. It is found in high amounts in meat, poultry, fish, eggs, and dairy products.
- Plant sources of methionine include nuts, seeds, legumes, and quinoa, but generally in lower quantities.”
- “Lysine: This amino acid is important for muscle growth, immune function, and collagen production. It is found in high amounts in meat, poultry, fish, and eggs.
- Plant sources of lysine include legumes, nuts, and seeds, but again, often in lower amounts than animal sources.”
- How Much Protein Do We Need? Stuart Phillips and Christopher Gardner
- Protein content and amino acid composition of … plant-based protein isolates
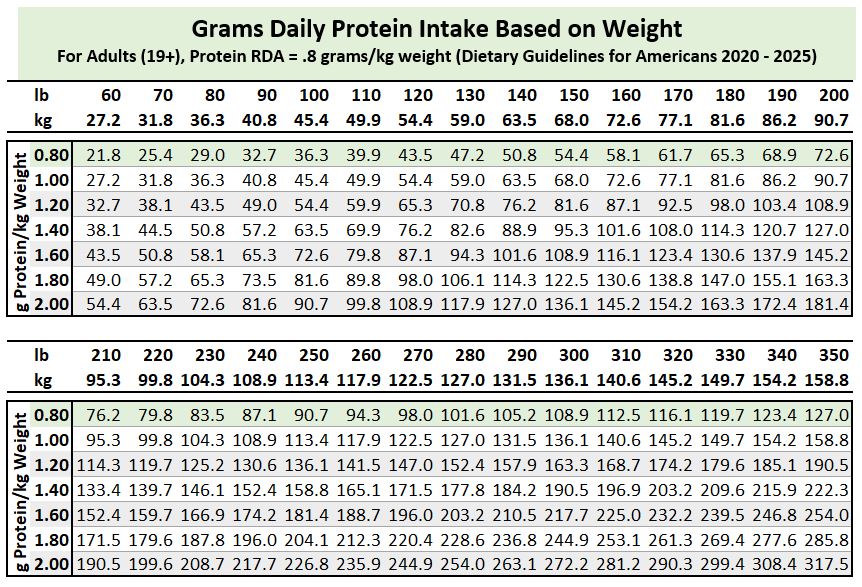
Protein Chart Based on g/kg Factor and kg (lb) Weight
- Example, for a 150 lb person, target protein for a .8 g/kg factor is 54.4 grams Protein.
- Example, for a 150 lb person, target protein for a 1.6 g/kg factor is 108.9 grams Protein.
My Approach to Protein
I am 61 now so ,for me, based on what I’ve read, it’s really important to make sure I am getting enough protein each day (since muscle loss starts happening …increasing?… as we age).
I like to lift weights and I’m trying to build on my strength. Strength is highly correlated with longevity i.e. you need to be able to grab things firmly, get up off the ground, etc.
Here’s what I have done to address my Protein needs:
- I tracked my protein intake over a month. I often did not meet the .8 g/kg wt. RDA.
- I am 61 and I am physically active. I therefore target about 1.6 g/kg (roughly a little over 100 g Protein/day). I might go higher over time.
- I take a protein powder supplement each day to help meet my daily target (~50 grams in the morning, sometimes more).
- As far as I know there is no Tolerable Upper Limit for Protein in the USA, so I am not worried about 1.6 g/kg being an unhealthy amount. Some of the experts recommend more than 1.6 g/kg.
Protein Resources/References
- I think you should always start with the NIH.GOV data: Nutrient Recommendations and Databases.
- https://www.dietaryguidelines.gov/
- Seek the opinions of the experts but read widely (sometimes hard to tell who the expert is).
- Find articles by or interviews with experts like:
- Peter Attia (MD)
- Christopher Gardner (PhD)
- Stewart Philips (PhD)
- Don Layman (PhD)
- Regardless of the source, keep your critical thinking “cap” on (see the tools in Appendix 2 to help you with that)
- Web articles and videos with a .gov or .edu tag.
- Podcasts produced by (or interviews with) Rhonda Patrick (PhD), Peter Attia (MD), Andrew Huberman (PhD) , Layne Norton (PhD) and Simon Hill (MSc) are informative as well.
- Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (2005)-Protein
- Dietary Reference Intakes: The Essential Guide to Nutrient Requirements (2006)-Protein
- NIH Factsheets – Exercise And Athletic Performance (for athletes 1.1 – 2 g/kg)
- Stanford.edu protein-needs-for-adults-50+ (1.2 – 1.6 g/kg)
- Harvard.edu how-much-protein-do-you-need-every-day
- Harvard.edu when-it-comes-to-protein-how-much-is-too-much (<=2 g/kg)
- Peter Attia (MD) – 2 g/kg aka 1 g/lb is recommended ; Kidney Toxicity might be an issue in the 3 to 4 g/kg range
- Protein “requirements” beyond the RDA (Stuart M Phillips, Stéphanie Chevalier, Heather J Leidy) 1.2 – 1.6 g/kg
Return Links
Omega-3 Fatty Acids
The Recommended Amounts (Adequate Intakes) for Omega-3 Fatty Acids for Adults
Men: 1.6 g (= 1,600 mg) as ALA (does not include EPA/DHA)
Women: 1.1 g (= 1,100 mg) as ALA (does not include EPA/DHA)
-
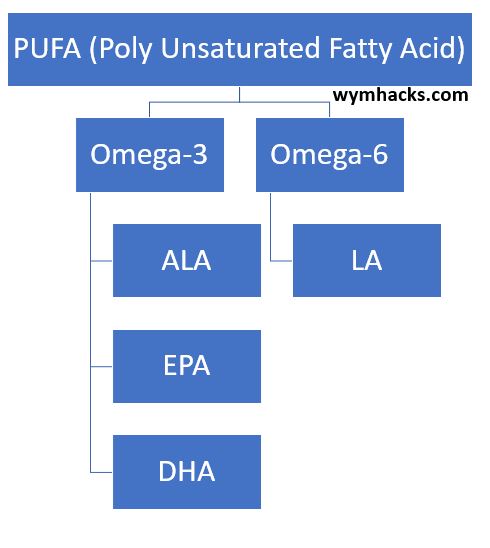
Per NIH: The three main omega-3 fatty acids are
- Alpha-Linolenic Acid (ALA) – Found in plants like flaxseed and soybean
- Eicosapentaenoic Acid (EPA) – Found in fish primarily.
- DocosaHexaenoic Acid (DHA) – Found in fish primarily.
-
Life Stage Recommended Amount of ALA (as Adequate Intakes or AI)
- “Birth to 12 months: *0.5 g
- Children 1–3 years: 0.7 g
- Children 4–8 years: 0.9 g
- Boys 9–13 years: 1.2 g
- Girls 9–13 years: 1.0 g
- Teen boys 14–18 years: 1.6 g
- Teen girls 14–18 years: 1.1 g
- Men: 1.6 g (= 1,600 mg)
- Women: 1.1 g (= 1,100 mg)
- Pregnant teens and women: 1.4 g
- Breastfeeding teens and women: 1.3 g
- * = As total omega-3s. All other values are for ALA alone.”
-
There are no Adequate Intakes established for EPA and DHA.
- AHA recommends two servings of seafood a week
- This roughly translates to a range of 240(avg.) to 575 mg (max) EPA + DHA..see below for how I computed this.
-
There are no Tolerable Upper Intake Levels for Omega 3 fatty acids.
- According to the Harvard School of Public Health (nutrionsource): The FDA “specifies that the labels of dietary supplements should not recommend a daily intake of EPA and DHA higher than 2000 mg due to lack of evidence.”
- NIH – Dietary Supplement Fact Sheets
- NIH – DRI (Daily Reference Intakes) Links
NIH: What are omega-3 fatty acids and what do they do?
According to the NIH:
- “Omega-3s (mainly ALA, EPA, DHA) are important components of the membranes that surround each cell in your body.”
- “DHA levels are especially high in retina (eye), brain, and sperm cells.”
- “Omega-3s also provide calories to give your body energy and have many functions in your heart, blood vessels, lungs, immune system, and endocrine system (the network of hormone-producing glands).”
- “Omega-3 fatty acids are found in foods, such as fish and flaxseed, and in dietary supplements, such as fish oil.”
- “ALA is found mainly in plant oils such as flaxseed, soybean, and canola oils. DHA and EPA are found in fish and other seafood.”
- “ALA, DHA, EPA are essential fatty acids, meaning the body must get them from food and cannot make them from scratch.”
PUFA (Poly Unsaturated Fatty Acids)
Lets provide some context around Omega-3 Fatty Acids.
- Lipids are a broad group of compounds that don’t readily dissolve in water
- PUFAs are a type of lipid (e.g. Fats or Phospholipids etc.) building block.
- PUFA molecules will contain long chains of carbon with more than one double bond.
- The PUFA structure causes kinks in the molecules and results in less dense packing.
- This characteristic (compared to saturated or single carbon bond Fatty Acids) is considered healthier (lower bad LDL, higher good HDL, etc.)
- Good healthier fats are the unsaturated fats.
- PUFAs consists of Omega-3 and Omega-6 Fatty Acids. These are essential fatty acids as the body cannot make them from scratch (must get them from food).
- Americans typically get more than enough Omega-6 (as LA) Fatty Acids (in vegetable oils, nuts, and even processed foods).
- Americans typically don’t get enough Omega-3 Fatty Acids.
Chart – PUFA Chemicals
So lets focus on the recommended amounts for the Omega-3 PUFAs.
Adequate Intake Amounts Don’t Include DHA and EPA
- The NIH (and associated organizations) don’t provide values for DHA and EPA.
- For ALA, you should be able to get your daily requirement from food (see the Chart below).
- I put about a tablespoon of ground flaxseed on my yogurt to cover my ALA requirements.
Table – Omega 3 ALA Content in food (Source: NIH Factsheet for Omega 3 Table 2)
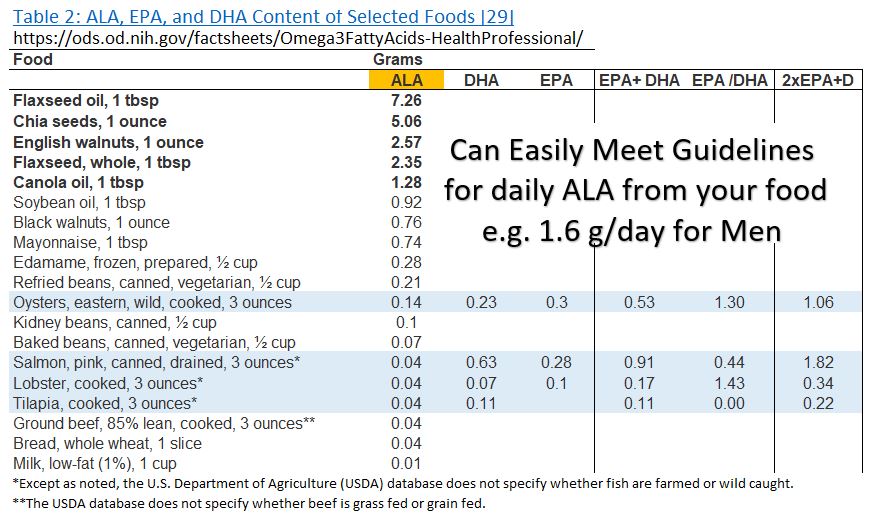
Now, what about EPA and DHA? Well, there are no Dietary Guidelines for these. But , we can back calculate some numbers based on the following:
- According to the NIH: “the American Heart Association (AHA) released three science advisories on omega-3s [66,88,89].
- All three advisories recommend one to two servings of seafood per week to reduce the risk of congestive heart failure, coronary heart disease, ischemic stroke, and sudden cardiac death, especially when the seafood replaces less healthy foods
- AHA Advice: American Heart Association: Are you getting enough omega 3 fatty acids?
From the dietary source table 2 provided in the NIH factsheet, I computed some rough averages and maximums for DHA + EPA in 2 servings of seafood a week.
- A daily intake of between 240 and 575 mg a day DHA + EPA covers the average and maximums from Table 2.
- You can check out how I computed this from the table below.
Table – Omega 3 DHA and EPA Content in food (Source: NIH Factsheet for Omega 3 Table 2)

Guidance from the AHA and Other Reputable Sources
Based on the American Heart Association’s article: Are you getting enough omega-3 fatty acids?
- “The American Heart Association recommends eating two servings of fish, particularly fatty fish, per week to help reduce heart disease and stroke risk.
- Two servings equal 6 ounces cooked.”
- Much higher levels of DHA and EPA might be safe and beneficial as well (2 to 3 g/day = 3000 mg/day) but AHA recommends assistance by your doctor.
According to the Harvard School of Public Health (nutritionsource):
- “Research strongly supports that eating a diet with fatty fish weekly provides protection from cardiovascular disease. However, many large clinical trials have not shown that taking omega-3 supplements provide the same protection”
- “The Food and Drug Administration specifies that the labels of dietary supplements should not recommend a daily intake of EPA and DHA higher than 2000 mg due to lack of evidence.”
- “For people with heart disease, the American Heart Association (AHA) recommends 1000 mg daily of EPA and DHA, preferably from fish, but supplements can be considered in consultation with a physician.” Note this is only for people with heart disease.
- “In specific cases, such as to lower triglycerides, the AHA recommends 2000–4000 mg daily of EPA and DHA under a doctor’s supervision.”
Notes from Readings and Listening
Note: The Advice given in these notes is not my advice; it’s advice from the podcast.
-
- Omega 3 – Get from Fatty Fish e.g. Wild Alaskan Salmon , Cod etc. – DHA, EPA are the marine versions of Omega 3 fats
- Bill Harris – Fatty acid Research Institute – Co-created the Omega 3 index – Measured in Red Blood Cells (better than plasma but longer lasting…120 days)
- Omega 3 index is a good marker for EPA and DHA in body.
- 8% or more is high, increases life by 5 years compared to lower (4%). On average is 5%. Japan has 10%.
-
Bill Harris – Omega 3 and Smoking Studies
- Non Smokers + High Index = highest life expectancy
- Smokers + Low Index = Lowest life expectancy
- But, Smokers + High Index Life Expectancy = Non Smokers + Low Index
- The type of fish matters. Avoid big fish (e.g. Swordfish) to avoid mercury, PCBs and other microcontaminants.
- Wild Salmon is better than farmed.
-
Most people don’t eat enough fish so supplements are an alternative.
- Take 2 grams a day.
- Raises you from a 4% to an 8% omega index (wym: I was not able to verify this. That’s a lot of daily supplements! )
- Make sure EPA and DHA supplements have low contaminant levels and low oxidation levels.
- It Matters how the supplements are made
- Use 3rd party testing sites
- https://www.consumerlab.com/
- https://www.iffo.com/ International Fish Oil Standard IFOS
- Find affordable brands with good EPA, DHA, Low oxidation level, Low contaminants
-
From Bill Harris (PhD) on Peter Attia(MD) Podcast
- Nice discussion on the organic chemistry nomenclature for Omega-6 and Omega-3 fatty acids.
- Omega refers to the last carbon in the fatty acid carbon chain.
- Omega 3 refers to the location of the double bond from the last carbon.
- It’s hard to predict the omega-3 index value from red blood cells relative to the diet you are on. This shows there is a lot of control and regulation going on in the body’s functions.
- Not all the studies have verified a connection between omega-3 supplements and reduction in chronic disease.
Major Studies and Study Reviews done on Omega 3 Supplements
Here is a sampling of studies. They don’t convince me that I need to take higher doses than the recommended guidelines for healthy people.
Higher doses (2 to 4 grams) is a lot of fish oil so this seems (to me) impractical not to mention expensive to do (especially when the understanding of the science behind it is not complete or comprehensive enough).
- Cochrane Reviews: Omega‐3 fatty acids for the primary and secondary prevention of cardiovascular disease
- Cochrane Reviews – Search for Omega 3 studies for other benefits
- VITAL Study (2018): This large-scale trial did not find a clear benefit for overall cardiovascular disease prevention but hinted at a possible reduction in heart attack risk
- REDUCE-IT Trial (2018): This large study demonstrated a significant reduction in cardiovascular events with high-dose (4 g/day) prescription omega-3s in high-risk individuals. There is some controversy around the Placebo set up.
- Omega-3 for Cardiovascular Diseases: Where Do We Stand After REDUCE-IT and STRENGTH? – Strength study and Reduce-it study have opposite conclusions.
Bottom Line On Omega-3 Guidelines
I agree with NIH’s recommendations which are excerpted below: Source:(NIH Omega-3 Supplements in Depth)
-
“How much do we know about omega-3 fatty acids (omega-3s)?
- Extensive research has been done on omega-3s, especially the types found in seafood (fish and shellfish) and fish oil supplements.”
-
“What do we know about the effectiveness of omega-3 supplements?
- Research indicates that omega-3 supplements don’t reduce the risk of heart disease. However, people who eat seafood one to four times a week are less likely to die of heart disease.”
- “High doses of omega-3s can reduce levels of triglycerides.”
- “Omega-3 supplements may help relieve symptoms of rheumatoid arthritis.”
- “Omega-3 supplements have not been convincingly shown to slow the progression of the eye disease age-related macular degeneration.”
- “For most other conditions for which omega-3 supplements have been studied, the evidence is inconclusive or doesn’t indicate that omega-3s are beneficial.”
-
“What do we know about the safety of omega-3 supplements?
- Omega-3s usually produce only mild side effects, if any.
- There’s conflicting evidence on whether omega-3s might influence the risk of prostate cancer.
- If you’re taking medicine that affects blood clotting or if you’re allergic to fish or shellfish, consult your health care provider before taking omega-3 supplements.”
What I do Regarding PUFAs
- Regarding ALA , I just add a tablespoon of ground flaxseed to my yogurt on most days.
- DHA and EPA come from fish, and the AHA recommends two 3 oz. servings a week.
- I usually don’t each fish, so I think it’s reasonable to supplement.
- My goal is to consume at least as much DHA and EPA as what is in 2 servings of fish.
- I (usually) take a daily fish oil pill that has 980 mg of DHA and EPA. The one I am taking is USP verified which gives me some level of comfort regarding its quality.
Omega-3 Fatty Acid References
- NIH: Omega-3 Supplements: In Depth – What’s the bottom line?
- NIH – Dietary Supplement Fact Sheets
- NIH – DRI (Daily Reference Intakes): Fatty Acids
- Rhonda Patrick interview with Shane Parrish
- Bill Harris (PhD) on Peter Attia(MD) Podcast
Return Links
Appendix 2 – Dietary Guideline Definitions of Terms
Before we get to the specific definitions, let’s understand the definitional framework:
- The DRIs (Dietary Reference Intakes) are the foundation (a comprehensive set of science-based reference values for nutrients).
- AMDR, RDA, EAR, UL, AI, and CDRR are specific terms within the DRI framework – each addressing different aspects of nutrient needs.
- The DGA (Dietary Guidelines for Americans) builds upon the DRIs.
- The DGA uses the scientific basis provided by DRIs to create practical dietary recommendations for the US population.
- So, the DRIs act as the scientific backbone, informing both the specific nutrient reference values within the system and broader dietary guidance like the DGA.
DRI (health.gov)
- Dietary Reference Intakes
- “A set of scientifically established reference values used for planning and assessing nutrient intakes of healthy people in the United States and Canada (Source: Health.gov)”
- “Dietary Reference Intakes (DRIs) are an important scientific underpinning to work related to nutritional health and safety at both the population and individual levels.
- The United States and Canada have collaborated since the mid-1990s to provide joint support for developing DRI values.
- The independent National Academies of Science, Engineering, and Medicine (NASEM) oversees this development process (Source: health.gov).”
RDA
- Recommended Dietary Allowance
- Daily nutrient intake sufficient for nearly all healthy individuals in a life stage group to prevent deficiency.
- The RDA is computed as the average requirement (EAR) plus 2 standard deviations.)
AI
- Adequate Intake
- Daily nutrient intake assumed to ensure nutritional adequacy for most healthy individuals when an RDA can’t be established.
EAR
- Estimated Average Requirement
- Daily nutrient level estimated to meet the needs of half the healthy population in a life stage group (serves as a benchmark for RDA).
UL
- Tolerable Upper Intake Level
- Highest daily nutrient intake level unlikely to pose risks of adverse health effects for most healthy people.
AMDR
- Acceptable Macronutrient Distribution Range
- Range of intake proportions for carbohydrates, protein, and fat considered adequate for most healthy people.
CDRR
- Chronic Disease Risk Reduction Level
- The estimated daily intake level for a nutrient that is expected to reduce the risk of developing chronic diseases within a seemingly healthy population.
DGA
- Dietary Guidelines for Americans
- The DGA is a set of evidence-based recommendations developed by the US Department of Agriculture (USDA) and the Department of Health and Human Services (HHS) every five years.
- The DGA provides general guidance for healthy eating patterns for Americans across all age groups.
A Few Other Terms and Equivalents (NIH)
- AT = alpha-tocopherol
- DFE = Dietary Folate Equivalent
- IU = International Units (specific to nutrient, see below)
- NE = Niacin Equivalent
- RAE = Retinol Activity Equivalents
Vitamin A
- μg= mcg = microgram = 1e-6 gram RAE
- 1 IU retinol = 0.3 mcg RAE
- 1 IU supplemental beta-carotene = 0.3 mcg RAE
- “RDAs for vitamin A are given as retinol activity equivalents (RAE) to account for the different bioactivities of retinol and provitamin A carotenoids, all of which are converted by the body into retinol.
- One mcg RAE is equivalent to 1 mcg retinol, 2 mcg supplemental beta-carotene, 12 mcg dietary beta-carotene, or 24 mcg dietary alpha-carotene or beta-cryptoxanthin”
Vitamin E
- mg = milligram = 1e-3 gram alpha-tocopherol
- 1 IU (natural) = 0.67 mg Vitamin E (as alpha-tocopherol)
- 1 IU (synthetic) = 0.45 mg Vitamin E (as alpha-tocopherol)
Vitamin D
- μg = mcg
- 1 IU = 0.025 μg
Folate
- μg = mcg
- 1 μg DFE = 1 μg Dietary Folate Equivalents
- 1 μg DFE = 0.6 μg folic acid
- The measure of mcg DFE is used because your body absorbs more folic acid from fortified foods and dietary supplements than folate found naturally in foods.
- Compared to folate found naturally in foods, you actually need less folic acid to get recommended amounts.
- For example, 240 mcg of folic acid and 400 mcg of folate are both equal to 400 mcg DFE.
Niacin
- mg NE
- 1 mg NE = 1 mg niacinamide
- 1 mg NE = 1 mg inositol hexanicotinate
- 1 mg NE = 1 mg niacin
- 1 mg NE = 60 mg tryptophan
- NE = Niacin Equivalents; Using mg NE accounts for both the niacin you consume and the niacin your body makes from tryptophan.