Part I. Chapter 1 – The Long Game
- You’re going to eventually die.
- {wymhacks: Bryan Johnson (Blueprint Protocol) believes that explosive non linear growth of human biological knowledge could very soon make step change impacts on human longevity.
- He’s been described as “eccentric”, but I think It’s worth a podcast or two to learn more about his measurement based learnings (and his protocols) }
- You’ll probably die from one of the following (1) Heart Disease (2) Cancer (3) Neurodegenerative Disease (4) Metabolic dysfunction
- Call them the “4 Horsemen”.
{wymhacks: Death Statistics}
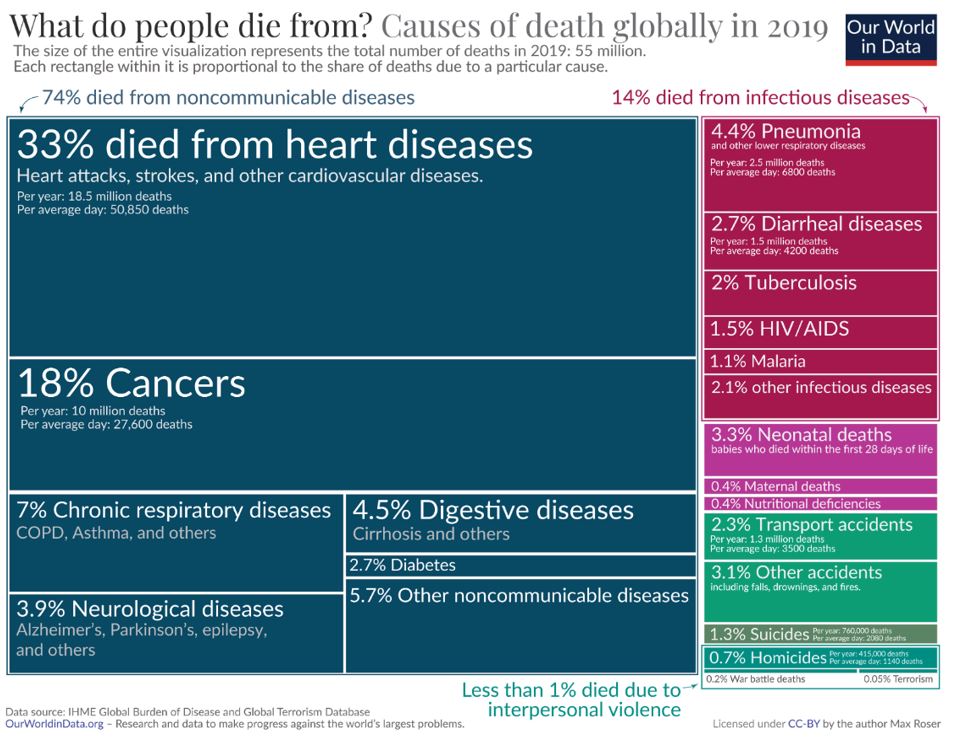
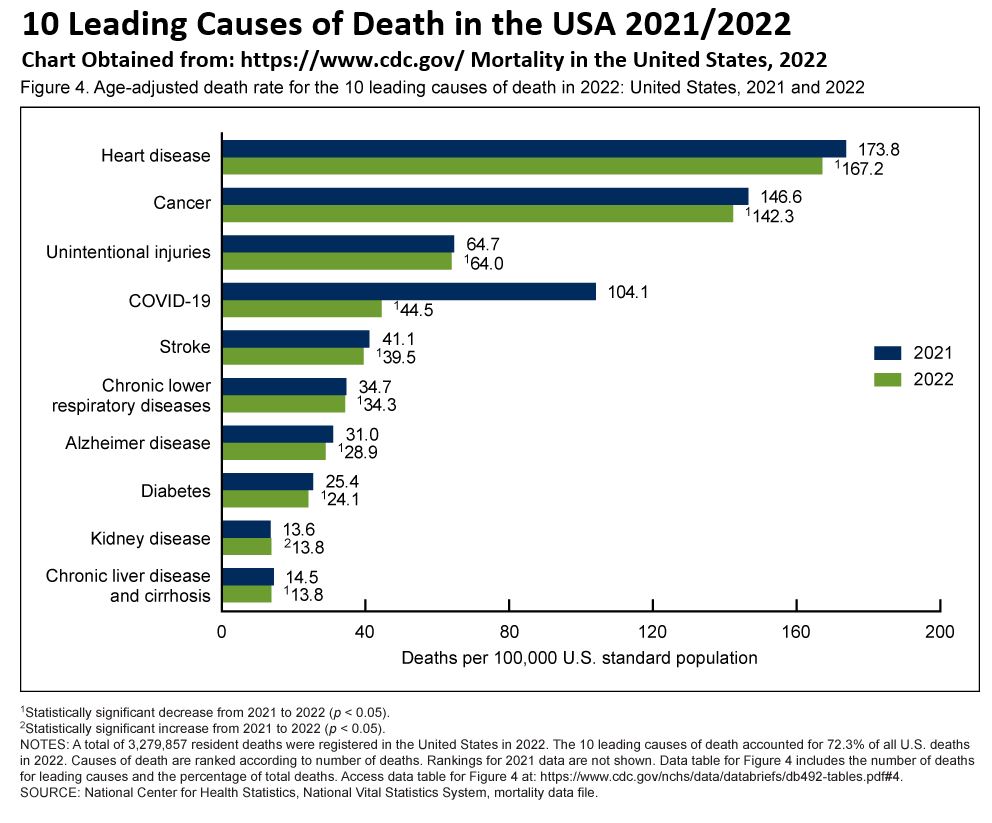
Check out the two charts below showing Global and USA causes of deaths.
Although Deaths from Diabetes are not at the top of the list, the book “Outlive” strongly makes the case that people with Diabetes (or are developing Diabetes) have an increased risk of dying from the other “Horsemen”.
Table_Causes of Death Globally in 2019 – Source: Our World in Data
Graph_10 Leading Causes of Death in the USA 2021/2022 – Source: CDC.gov
- Traditional medicine has been most effective at preventing “fast death” from injuries, infections etc.
- Traditional medicine has not been as effective against “slow death” from the “4 Horsemen”.
- “Slow death” timeline includes development and progression of the disease which probably has taken years before symptoms are felt or detected.
- “We need to step in sooner to stop the 4 Horsemen in their tracks”
- Consider Type-2 Diabetes
- Normal blood glucose is 100 mg/dL ; Hemoglobin A1c (HbA1c) = 5.1%
- Only when blood glucose >=140 mg/dL (HbA1c >=6.5%) do ADA standard-of-care treatment guidelines kick in.
- A measurement slightly less (e.g. HbA1c =6.4%) results in less rigorous treatment (Pre-Diabetes).
- But even Pre-Diabetes is an almost “end of the line” symptom that took a long time to develop.
- This is not the proper approach. It should not be treated like a “cold or a broken bone”.
- Action should be taken way before any “end of the line” symptoms appear.
- The focus of this book is to advocate for a proactive approach to longevity with the goal of
- increasing Lifespan (living longer) but also
- increasing Healthspan (higher quality of living, especially the back end years).
Part I. Chapter 3 – Objectives, Strategy, Tactics
Objective
Medicine 2.0 intervenes too late.
- The duration from the intervention to death could be low quality (painful etc.).
Ideally, in Medicine 3.0, you live a high quality life for most of your life; and in the end your quality of life drops quickly and you die quickly.
- So, you suffer less in those last years.
“Outlive” applies an Objective – Strategy – Tactic approach.
The Objective is to delay death and to get high quality years while doing it (live longer and better).
- i.e. optimal Healthspan and longevity
Picture – Ideal life is a Steep and Quick Demise (long Healthspan)

Strategy
Part II of the book is dedicated to Strategy.
Strategy: To gain a deeper understanding of the science and evidence surrounding
- The 4 Horsemen
- Aging
- Healthspan deterioration
- Cognitive decline
- Loss of physical function (see “activities of daily living” checklist)
- Emotional health
Tactics
Part III. of “Outlive” is dedicated to Tactics
Medicine 2.0 tactics:
- Procedure (e.g. surgery)
- Medications
Medicine 3.0 tactics:
- Exercise
- Nutrition
- Sleep
- Emotional health
- Exogenous molecules (drugs, hormones, supplements) – not covered in this book (too big of a topic)
“Outlive” Uses an Evidence Informed (vs Based) Strategy
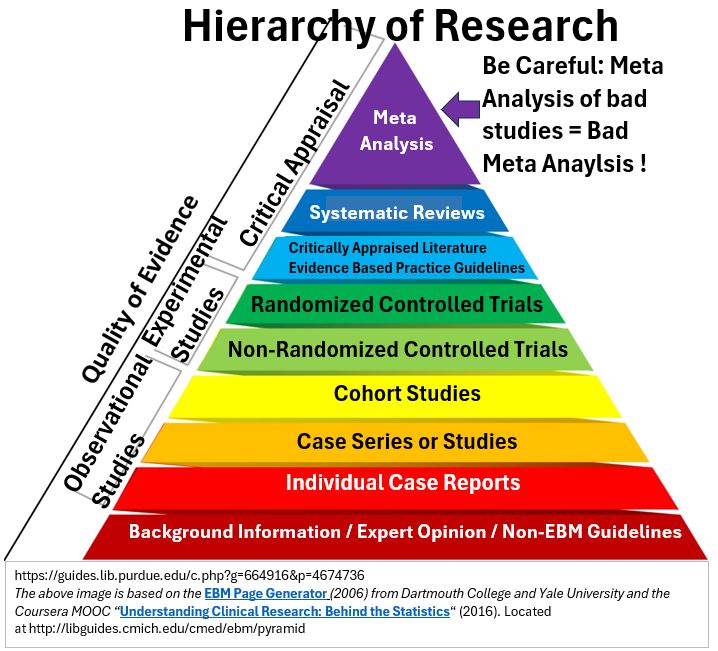
Randomized Controlled Trials (RCTs) are the gold standard but are difficult to apply to the long durations and complex interventions regarding the 4 Horsemen.
{wymhacks – Pyramid Graph – Hierarchy of Research}
- {wymhacks: if you want to learn more about evaluation techniques refer to https://pubmed.ncbi.nlm.nih.gov/
- and search for a 32 part series that has the common title of “….part XX of a series on evaluation of scientific publications”.
- RCTs are discussed in part 17. }
- {wymhacks: See https://peterattiamd.com/ama30/
- and https://peterattiamd.com/ns004/ }
“Outlive” uses an evidence informed approach and combines insights from 5 sources:
- Study of centenarians – observational not experimental
- Lifespan data from animal models (e.g. mice)
- Human studies of the 4 Horsemen
- Molecular and mechanistic insights from aging studies
- Mendelian Randomization (MR)
- {wymhacks: MRs Compare people with genetic differences that cause a certain thing.
- e.g. People with gene defect that doesn’t break down toxin when toxin is introduced versus people with same gene defect not exposed to toxin}
- {wymhacks: https://www.cdc.gov/genomics/disease/mendelian_randomization.htm }
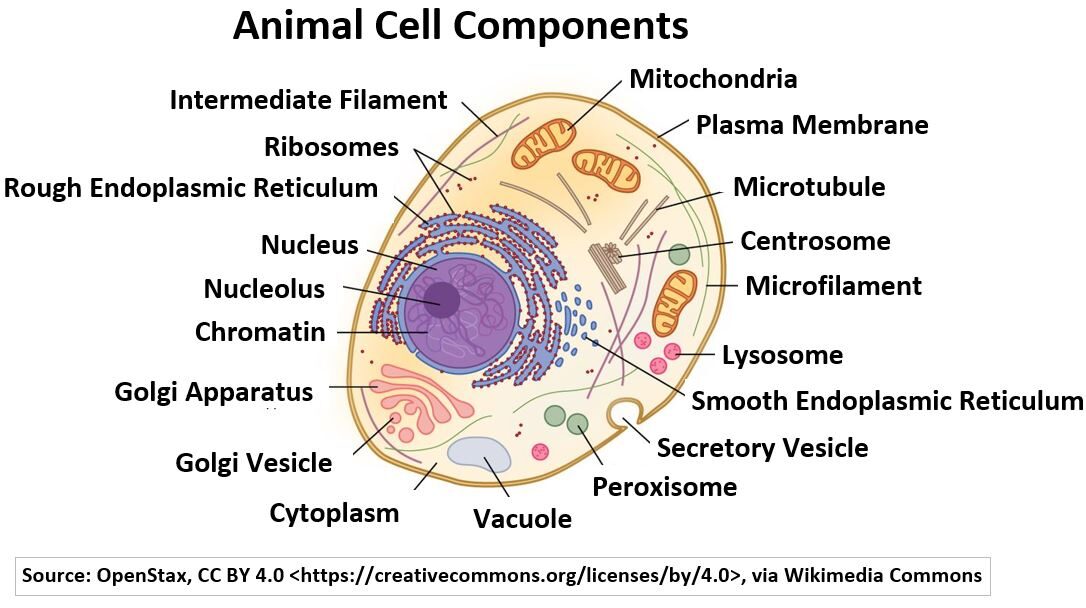
{wymhacks – Human Cell Components}
To understand the human body you need to start with the structure of the cell.
Most cells of the body will contain the components shown in the schematic below.
Picture_Animal Cell Components
You can refer to my post linked below for a refresher:
Human Cell Structure and Components
Here’s a brief summary of some of the key components (organelles) within human cells that are crucial for energy / metabolism and genetics:
note: I used Google Gemeni to construct the below sentences (regarding cell organelles).
Mitochondria are
- “powerhouses” of the cell that are central to metabolism.
- responsible for cellular respiration (the process that generates energy from Nutrients).
The Nucleus
- houses the cell’s DNA, which contains the genetic code.
- controls gene expression (regulate protein synthesis, which is essential for all cellular functions).
Ribosomes
- are the protein synthesis factories of the cell.
- play a key role in metabolism (Since they make proteins called Enzymes, which catalyze metabolic reactions).
- play a role in translating genetic information into proteins.
Endoplasmic Reticulum (ER) and Golgi Apparatus
- are involved in protein processing, modification, and transport.
- take part in the production of proteins needed for metabolism and
- play a role in lipid and carbohydrate metabolism.
Cytoplasm is
- the gel-like substance inside the cell that contains all the organelles.
- is the site of many metabolic reactions.
The Cell’s organelles work together to
- maintain the cell’s energy levels,
- carry out metabolic processes, and
- ensure the accurate transmission and expression of genetic information.
{wymhacks – Genetics Refresher}
A full ‘set’ of 46 Chromosomes are located in almost all your cells of which you have Trillions (30 Trillion according to this source).
Picture_Genetic Material Simplified Drawing
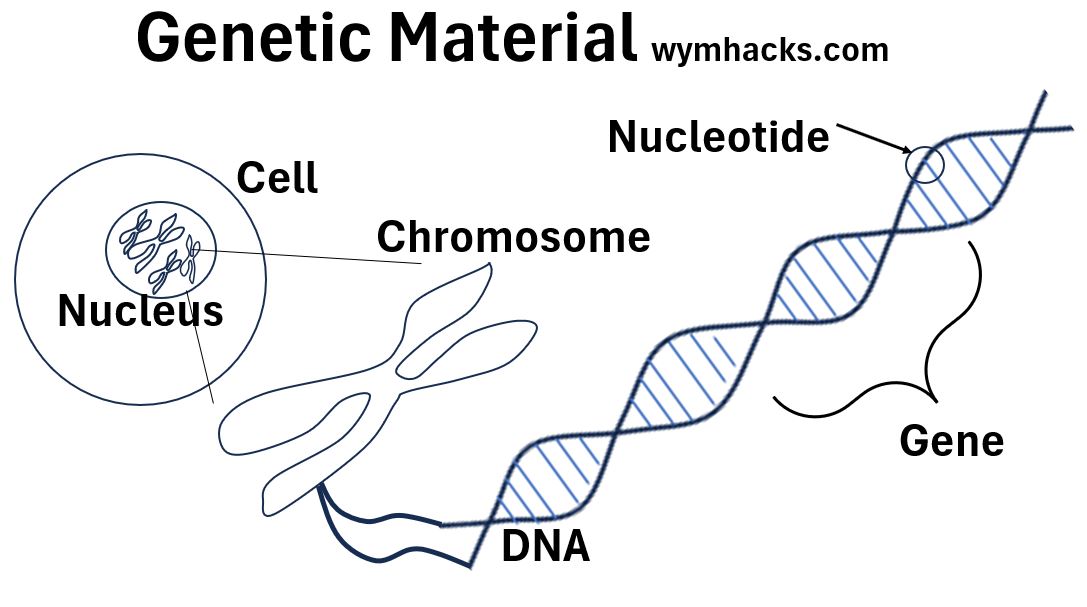
You should learn a little bit about genetics.
According to the CDC,
- “Genes play a role in almost every human trait and disease.”
- “Advances in our understanding of how genes work have led to improvements in health care and public health.”
So click on the link to my post below and learn!
Genetics Basics
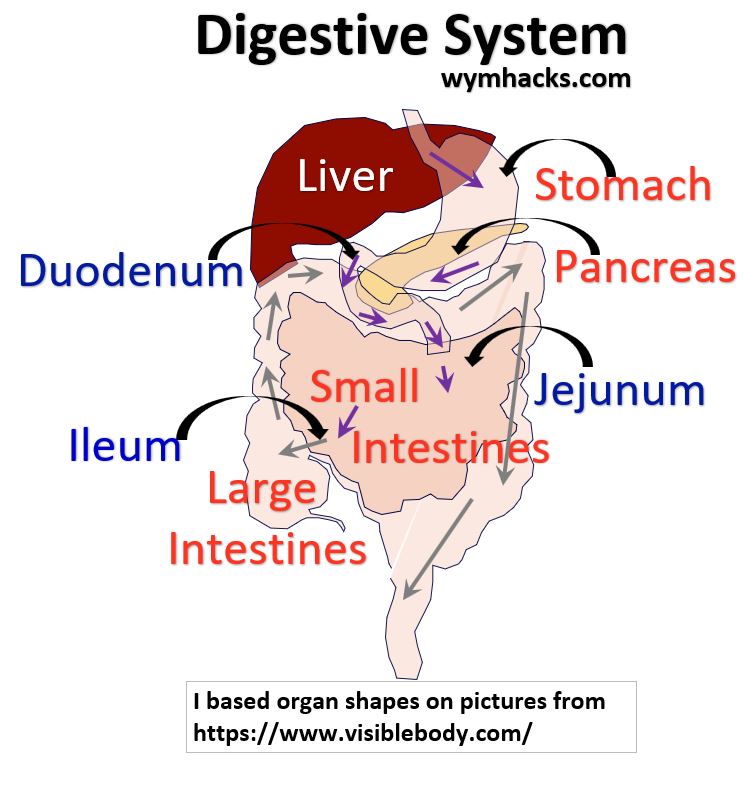
{wymhacks – Metabolism Defined}
Metabolism can be broadly defined as “chemical reactions that occur in the body that support / sustain / maintain life”.
We eat food and our Gastro Intestinal (GI) Tract breaks it down and utilizes the micro-components in various ways.
Picture_Digestive System (Gastro-Intestinal Tract)
Read my introductory post,
Metabolism Defined
In this article, I introduce Metabolism in the context of the
- breaking down of nutrients (Catabolism),
- energy production (Cellular Respiration), and
- molecule building (Anabolism).
We can’t introduce Metabolism without talking about ATP.
So , let’s do that now.
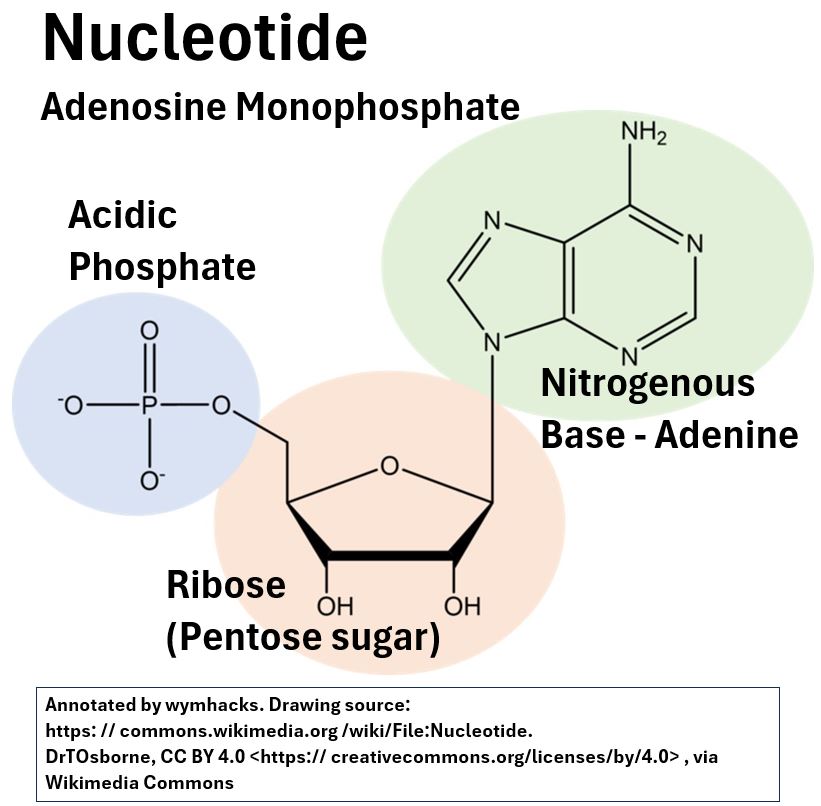
{wymhacks – ATP – Adenosine Triphosphate (Tri-Phosphate)}
Adenosine Triphosphate (ATP) is the “energy currency” of the cell because it contains the energy needed to fuel cellular processes.
Picture_Adenosine Tri-Phosphate (ATP) C10H16N5O13P3
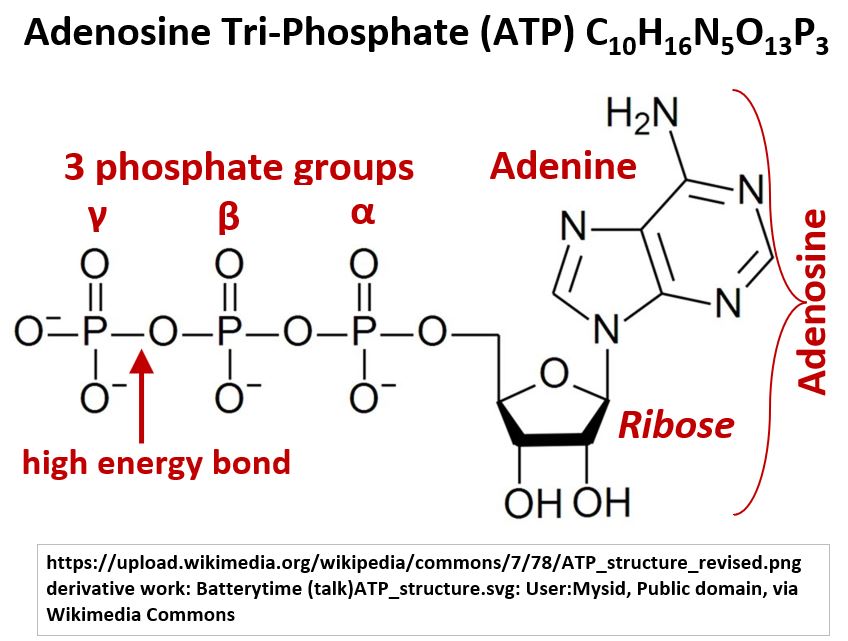
ATP (along with RNA and DNA) are the rock stars of the biochemical world (there are a few others we’ll discuss later).
ATP has 3 phosphate groups, a Ribose (sugar) group, and a nitrogenous base (Adenine).
We’ve seen a structure very familiar to this already.
Yes!, that’s right, ATP is a three phosphate version of the single phosphate nucleotide we see in an RNA molecule.
Picture_RNA Nucleotide
Link to my post below, and learn more about this amazing molecule’s structure and hydrolysis by water.
ATP (Adenosine Triphosphate)
Also, check out this great general description of ATP by Sal Khan:
We said that ATP is the energy currency of the cell.
Cellular Respiration is the process by which cells generate ATP by breaking down glucose and other molecules.
So, let’s take a closer look at Cellular Respiration.
{wymhacks – Cellular Respiration}
![]()
I’ve written separate posts for each stage of Cellular Respiration.
You can access these via the links below as well as view a general summary of each stage.
Cellular Respiration (I) Overview
Cellular Respiration is a metabolic process that occurs (mostly) in the Mitochondria of cells to produce ATP, the primary energy source for cellular processes.
Through four major chemical reaction stages, roughly 32 molecules (30 – 32) of ATP are produced for each molecule of Glucose.
- Glycolysis breaks down molecules and generates energy carrying molecules like NADH and ATP.
- Pyruvate reacts to Acetyl CoA which enters the Krebs Cycle.
- The Krebs Cycle builds up and breaks down molecules to generate more energy carrying molecules like NADH, FADH2, and ATP.
- Oxidative Phosphorylation (Electron Transport Chain and Chemiosmosis) takes the energy from NADH and FADH2 and creates (a lot) more ATP.
Cellular Respiration (II) Glycolysis
Glycolysis is a metabolic pathway that breaks down simple sugars into Pyruvate molecules.
These reactions occur in the cytoplasm of cells and don’t require oxygen.
Glycolysis produces 2 NADH and 2 ATP.
The NADH is an electron carrier and is used in the last stage of Cellular Respiration to make more ATP.
Cellular Respiration (III) Pyruvate to Acetyl CoA
Stage 2 of Cellular Respiration is called the Transition Step,
- where 2 Pyruvates (produced for each Glucose) are converted to 2 Acetyl CoA molecules, and where
- 2 NADHs and 2 CO2s are also produced.
Acetyl CoA is a versatile Nucleotide containing molecule:
- It delivers an Acetyl group to the 3rd Stage of of Cellular Respiration, the Krebs Cycle.
- Acetyl CoA also plays a role in other metabolic pathways (e.g. biosynthesis involving Fatty Acids and Amino Acids etc. )
Cellular Respiration (IV) Krebs Cycle
The Krebs Cycle, the 3rd Stage of Cellular respiration, produces, per molecule of glucose,
- 2 ATP
- 6 NADH and
- 2 FADH2
FADH2 is yet another important Adenine Nucleotide molecule. The NADH and FADH2 molecules are electron carriers to be used in the 4th and final stage of Cellular Respiration.
Cellular Respiration (V) Oxidative Phosphorylation
The majority of ATP, the powerhouse cell of the body, is produced by Oxidative Phosphorylation.
This occurs in the final stage of Cellular Respiration.
The Oxidation occurs to the electron carriers NADH and FADH2 which are produced in the earlier phases of Cellular Respiration.
The released electrons move through a series of proteins , resulting in the creation of a proton gradient between the Mitochondrial Matrix and the Intermembrane of a Mitochondrion.
This is sometimes described as the Electron Transport Chain.
At the end of the electron cascade, electrons react with hydrogen and oxygen to form water.
Through Chemiosmosis of the protons through the enzyme ATP synthase, ATP is produced from the Phosphorylation of ADP.
For every molecule of Glucose about 27 to 38 molecules of ATP are formed.
References
{wymhacks – Metabolic Pathways}
The chemical reactions that run and maintain life are varied and often interrelated.
Collectively we describe these as Metabolism.
The core mechanism of Metabolism is the Cellular Respiration reaction pathway.
It is sometimes described as Central Metabolism because practically all metabolic paths for different nutrients pass through it or are connected to it in some way.
That is,
- Carbohydrates, Proteins, and Fats can all undergo Cellular Respiration to produce energy, but
- they can all be used to create molecules as well.
Picture_Metabolism
For an in depth exploration of Central Metabolism and its many reaction pathways, please click the link below.
Metabolic Pathways
This article will teach you that the Cellular Respiration Pathway
- serves as a central hub for several critical biochemical reactions.
- allows your body to extract energy not only from carbohydrates (e.g. Glucose) but also from Proteins (Amino Acids) and Fats (Glycerol and Fatty acids).
- “intermediates” also play critical roles in anabolic processes (i.e. building molecules needed for life like tissues, organs, enzymes, hormones etc.)
On the surface it seems relatively simple…You ingest nutrients and oxygen and you reject carbon dioxide, water, and waste.
But all the time, an incredibly complicated blend of biochemical reactions are going on in your body.
The reactions are tightly regulated and controlled (via enzymes and hormones) to ensure your body stays alive and nourished.
Part II. Chapter 6 – The Crisis of Abundance
Ok, back to Attia’s book “Outlive” (Part II. Chapter 6).
NASH
- 1980s: Mayo Clinic named it: NonAlcoholic SteatoHepatitus {wymhacks: NASH}.
- It’s the progressive form of its precursor, Non Alcoholic Fatty Liver Disease {wymhacks: NAFLD}.
- So, NAFLD -> NASH
- NASH can cause inflammation, scarring of the liver and could lead to Cirrhosis. {wymhacks: See liverfoundation.org for more on NAFLD and NASH}.
- So, NASH is not caused by alcohol.
- It’s Caused by too much fat buildup in liver.
- NAFLD / NASH is highly correlated with obesity and high cholesterol {wymhacks: hyperlipidemia}.
- No obvious symptoms make this dangerous.
- Blood ALT test (for liver enzyme alanine aminotransferase) might pick it up but not in the early stages.
Acceptable ALT range:
- <33 IU/L (women); IU = International Unit
- <45 IU/L (men).
- These might be too high.
- You might have an unhealthy liver even if these numbers are lower.
- The Liver is a resilient and regenerative organ.
- You can reverse effects of NASH and NAFLD (up to a point ; most commonly by weight loss)
- NAFLD / NASH are the “tip of the iceberg of a global epidemic of metabolic disorders,
- ranging from Insulin Resistance to Type-2 Diabetes.”
- {wymhacks: Insulin Resistance – Muscle / Fat/ Lever cells can’t efficiently take up glucose from your blood or store it}
- {wymhacks: Type-2 Diabetes – chronic condition of high blood sugar levels (Hyperglycemia). }
Type-2 Diabetes is the “last stop on a railway line passing through”
- Hyperinsulinemia (high insulin in blood)-> Pre-Diabetes -> NAFLD / NASH
- If you are anywhere on this disease “train”, you are susceptible
- to the other Horseman diseases (Cardiovascular Disease, Cancer, Alzheimer’s Disease).
- {wymhacks: According to liverfoundation.org ,
- “Nonalcoholic fatty liver disease tends to develop in people who are overweight or obese or have diabetes, high cholesterol, or high triglycerides.
- These conditions combined are known as Metabolic Syndrome.”}
- {wymhacks: Metabolic Dysfunction is a broad term describing one or more abnormal metabolic issues involving:
- breaking down nutrients,
- using nutrients for energy,
- disrupted or abnormal enzymatic or hormonal activity
- etc. }
- { wymhacks: Metabolic Dysfunction/s lead/s to Metabolic Syndrome (and/or other isolated effects):
- For example, Insulin Resistance is a Metabolic Dysfunction that leads to
- high blood Glucose, which is a Metabolic Syndrome.}
Obesity
- According to CDC, > 40% of US population is obese (BMI; Body Mass Index >30).
- Another 30% are overweight (BMI 25-30)
- An Obese person has a higher risk for chronic disease.
- Obesity is one symptom of a Metabolic Dysfunction like hyperinsulinemia (high blood insulin).
- But,
- Not everyone who is obese is metabolically unhealthy and
- Not everyone who is metabolically unhealthy is obese
Metabolic Syndrome (MetSyn)
- A 1980s concept by Gerald Reaven at Stanford. Named MetSyn eventually.
- Metabolic Syndrome or MetSyn defined in terms of the following criteria:
- Criteria 1: High blood pressure (>130 / 85 mm mercury)
- Criteria 2: High triglycerides (>150 mg/dL)
- Criteria 3: Low HDL cholesterol (<40 mg/dL in men, <50 mg/dL in women)
- Criteria 4: Central adiposity (waist circumference > 40 inches in men and > 35 inches in women)
- Criteria 5: Elevated fasting glucose (>110 mg/dL)
- {wymhacks: A mg (milligram) is 1000th of a gram and a dL (deciliter) = 100 cubic centimeters = a cube with 4.64 cm sides or 1.83 inch sides (basically a cube that fits comfortably in your hand)}
IF YOU MEET 3 OR MORE OF THESE CRITERIA, THEN YOU HAVE METABOLIC SYNDROME
- Each of these criteria can be described as a Metabolic Dysfunction.
- Possibly 100s of millions of American adults have Metabolic Syndrome.
- {wymhacks: One article claims that “ Less than one-third of normal weight adults were metabolically healthy and the prevalence decreased to 8.0% and 0.5% in overweight and obese individuals, respectively.”}
- {wymhacks: According to this article, about ∼20% of the normal weight adult population is metabolically unhealthy.
- So metabolic dysfunction affects non-fat people as well.}
- So understand it’s not only obesity that increases the risk of bad health outcomes.
- More broadly, Metabolic Dysfunctions increase the risk of bad health outcomes.
- {wymhacks: According to the NIH, “Metabolic syndrome is a group of conditions that together raise your risk of
- coronary heart disease,
- diabetes,
- stroke, and
- other serious health problems.”}
{wymhacks: Causes and Risks of MetSyn}:
- Being inactive,
- Eating an unhealthy diet and large portion sizes,
- Not getting enough good quality sleep,
- Smoking,
- Drinking a lot of alcohol,
- Shift work.
Carbohydrate Metabolism
{wymhacks – Carbohydrates according to my.clevelendclinic.org are fibers, starches and sugars that your body converts into glucose (blood sugar) to give you the energy you need to function.}
Metabolism is the “process of taking in nutrients and breaking them down for use in our body.”
Let’s understand how our body metabolizes carbohydrates (or carbs for short).
Route 1 – Carbs Converted to Glycogen (For Near Term Use)
{wymhacks: Glycogen is a polymer ,i.e. repeating subunits, of glucose}
75% of glycogen ends up in muscle, and 25% of glycogen to the liver.
About 1600 calorie capacity between these two sites
- {wymhacks: Not A lot! If I’m swimming, calorie use might be 280×2 = 560 cal/hr = 1120 for 2 hours}
- {wymhacks: a thermal kcal (kilo calorie or 1000 calories) is equal to a dietary Calorie.
- So, technically 1 dietary Calorie = 1 kilo calorie or kcal.
- A kcal is the amount of energy required to raise the temperature of 1 kg of water one degree centigrade at sea level.}
- {wymhacks: Protein and Carbohydrates contain ~4 kcal/g
- Pure fat contains ~9 kcal/g
- Technically adipose tissue is not 100% fat so the heat content of adipose will be less than 9). }
The Liver maintains glucose balance in the blood.
- Called Glucose Homeostasis
- The average adult male has only 5 grams (1 teaspoon) of glucose in blood.
- Glucose is used up quickly by muscles and brain, so the liver is essentially continuously squirting converted glycogen (glucose) into the blood.
- 7 grams of glucose in blood means you have Diabetes!!! This is a very delicate balance.
Route 2 – Carbs Converted to Fat (for Energy Storage)
Unlike our limited glycogen capacity, we have a lot of fat capacity.
- A Relatively lean adult could be carrying 10 kg of fat (3500/lb x 2.205 lb/kg x 10 kg = 77,175 calories)
- Compare that to 1600 calories.
- That is, our energy from fat storage capacity is ~ 48x the capacity of energy storage via glycogen.
{wymhacks: Hormone Primer}
I think you’ll appreciate the following sections on Insulin and Glucagon much more if you first review these great references.
The Pancreas Maintains Glucose Homeostasis in the Blood
- The body senses Glucose levels in the blood and the Pancreas releases Insulin to control it.
- Intense exercise results in immediate uptake of glucose by your muscles whereas
- being sedentary results in Glucose conversion to Fat.
- Fat is not bad fundamentally (depends on where it is)
- Subcutaneous (under skin) fat is safest place to store energy
- Subcutaneous fat plays an important role in maintaining metabolic health
- Fat is like a “metabolic buffer zone”.
- The body safely uses it for energy storage and extracts energy from it as needed
{wymhacks: Additional notes on Insulin and Glucagon}
- Read my post Metabolic Pathways.
- The Pancreas Islets of Langerhans secrete two hormones:
- Insulin: reduces blood glucose and
- Glucagon: increases blood glucose.
From khanacademy.org
- The body maintains glucose in blood between 70 and 120 mg/dL.
- A mg is 1000th of a gram.
- A dL = deciliter = 100 cubic centimeters = a cube with 4.64 cm sides or 1.83 inch sides.
- Too high, you could get Hyperglycemia (eye, nerve, kidney disease….i.e. diabetes).
- Too low you get Hypoglycemia (fatigue and worse).
- To Reduce Glucose in Blood, Insulin Initiates Conversion of
- Glucose to energy via Glycolysis
- Glycolysis – First phase of how your body extracts energy from glucose.
- Glucose to Glycogen (polymer of Glucose) via Glycogenesis in the liver and muscle and
- Glucose to Lipids (fats are one form of lipid)
- This is a multi-step process resulting in Fatty Acids
- Glucose-> Pyruvate-> Acetyl-CoA-> Fatty Acids
- Fatty acids react to form fat (triglycerides or TAGs) by Lipogenesis.
- In a Fasting State, Fatty Acids can also convert to Ketone Bodies
- Ketone Bodies are other energetic molecules
- Usually stored in adipose or fat tissue of body.
- Sometimes called De Novo Lipogenesis.
- Glucose to energy via Glycolysis
Fat Storage in The Body (Bathtub Analogy)
Consuming energy in excess of your needs eventually
- Exceeds the capacity of subcutaneous fat and
- Results in fat “spillover” into other bodily regions.
{wymhacks – see the picture below showing a bathtub analogy of this energy balance.}
{wymhacks – Picture_Bathtub Analogy of Bodily Fat (Energy) Balance}
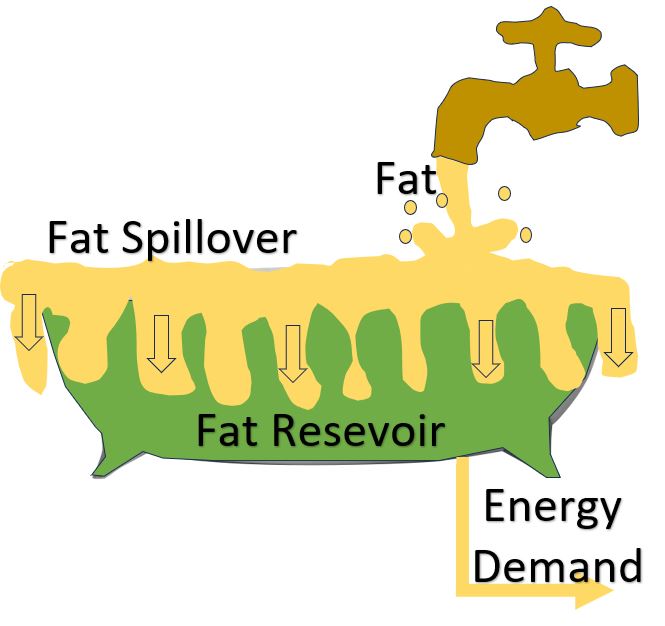
- Eventually results in the subcutaneous fat reservoir (the bathtub) overfilling.
- Subcutaneous fat capacity differs widely among individuals.
- Possibly influenced by genetic factors.
- e.g. Asian subcutaneous fat capacity much lower than Caucasian capacity
- One explanation for why some people are “skinny” but still have metabolic dysfunctions.
- Suggests that having some fat versus being leaner might offer some metabolic protection.
- When the “reservoir” is full, fat spills over into various organs and tissues
- Like the liver, heart, muscles, kidneys, pancreas, and visceral regions.
- This fat buildup can cause NAFLD, insulin resistance and inflammation
- The Pancreas’s ability to secrete insulin can be impaired and lead to Type-2 Diabetes.
- Visceral fat (accumulating among the organs) can be dangerous.
- Inflammatory Cytokines (TNF-alpha, IL-6) are released. (see my post: The Immune System – A Primer)
- Cytokines are key markers and drivers of inflammation.
- It’s linked to cancer and cardiovascular disease
Visceral Fat
If you have 20% body fat and about 11% or of that is visceral fat, you might be at high risk for cardiovascular risk and Type-2 Diabetes.
- Attia patients take annual DEXA scans to determine visceral fat
- DEXA determines bone density, visceral fat, body fat, and muscle mass
Insulin Resistance
One of the first places fat-overspill will go to is your muscles.
- like marbling in a steak!
- Insulin Resistance likely begins here and spreads to organs like the liver
- This Fat disrupts cellular insulin transport mechanisms
- Inactivity (lack of physical activity) enables/speeds this process
Insulin Resistance means cells, initially muscle cells, stop responding to insulin’s signals.
- Cellular Glucose uptake eventually decreases.
- The Pancreas responds by injecting more insulin
- Eventually (fasting) blood glucose begins to rise (as well as insulin)
- The Pancreas can eventually fatigue.
- All the while more fat is being produced (remember insulin enables glucose to fat conversion)
- Many hormones affect fat distribution and fat use but Insulin is the big one
- Cortisol release caused by stress and lack of sleep can also contribute to visceral fat accumulation
- High insulin (Hyperinsulinemia) results in
- Fat gain
- Increase risks for atherosclerosis and cancer
- On the way to Type-2 Diabetes
Type-2 Diabetes
The “disease of civilization”.
- {wymhacks: Type-1 Diabetes is much less prevalent (maybe 5% of total Diabetes Cases)}.
- {wymhacks: Type-1 Diabetes: The body can’t make insulin, usually starting in childhood.}
- {wymhacks: Type-2 Diabetes is the most common type of Diabetes (90% to 95% of Diabetes cases)
- With Type-2 Diabetes, the body doesn’t use insulin properly
- It’s linked to lifestyle factors
- Type-2 Diabetes is more common in adults and is sometimes called Adult Onset Diabetes. }
- (2022 CDC) – Over 11% of US adult population (1 in 9) has type-2 Diabetes
- Over 29% of adults over 65 have it.
- Almost 50% of adult population is pre-diabetic or has Type-2 Diabetes
- Patients with Diabetes have a much greater risk of cardiovascular disease, cancer, Alzheimer’s and other Dementias
- Why is this epidemic happening?
- (Possibly) Our metabolism, evolved over millennia, cannot cope with our modern diet.
- The environment has changed much faster than our Genome.
- Evolution still wants us to get fat (not so useful in our era of unlimited calories)
Fructose
Let’s talk Fructose. See my post Fructose Metabolism Chart also.
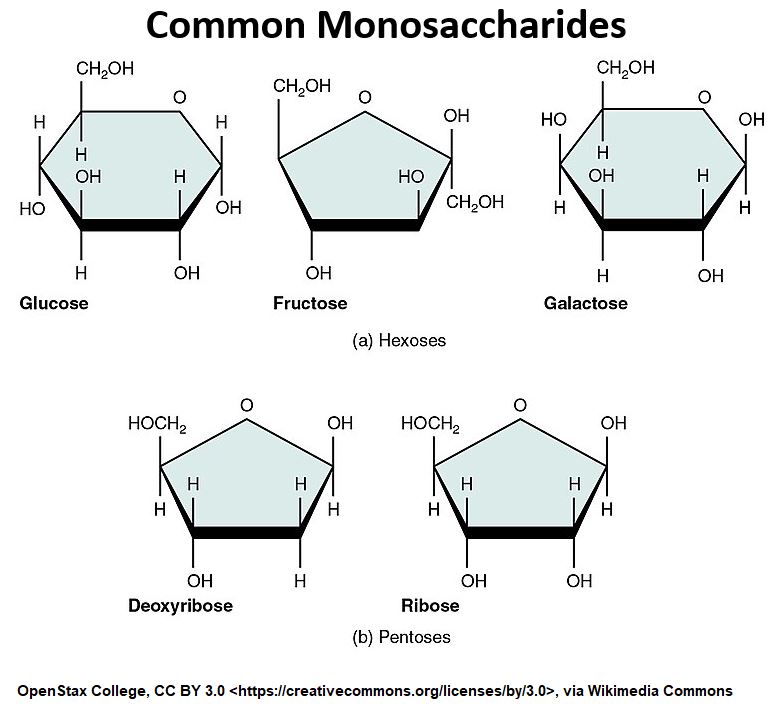
Fructose is the common sugar found in , you guessed it, fruits. It has the same molecular formula as Glucose but has a different structure (they are isomers of each other).
{wymhacks: Fructose is one of a number of monosaccharides. You’ve already seen some of these and know how important they are
- DNA and RNA molecules contain deoxyribose and ribose sugar groups
- Glucose is a key energy source for most cells in the body (the brain needs glucose) }
{wymhacks – Picture_Common Monosaccharides}
{wymhacks: See the simple picture showing Fructose metabolism below.
Recall that the Cellular Respiration pathway is described as Central Metabolism because practically all metabolic paths for different nutrients pass through it in some way. }
{wymhacks – Picture_Cellular Respiration Pathway with Fructose Entry Point}
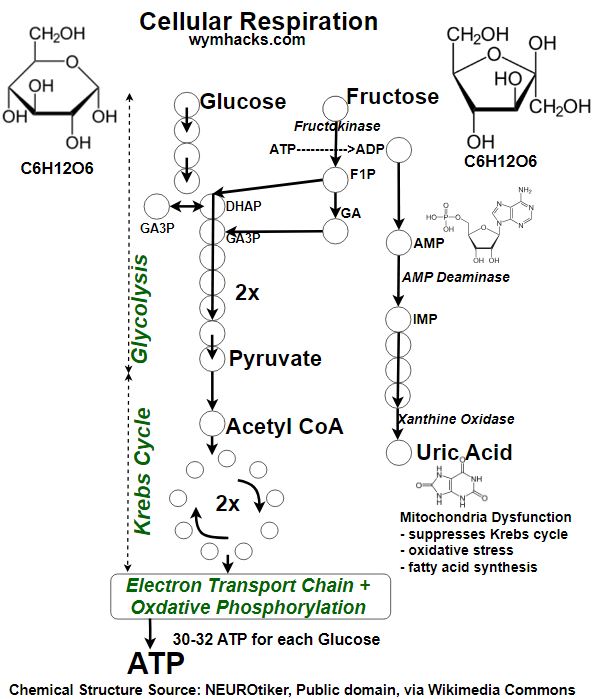
- Dihydroxyacetone phosphate (DHAP)
- Glyceraldehyde 3-phosphate (G3P)
But the more interesting (and dangerous route for humans) is the production of Uric Acid.
- Fructose is directly phosphorylated to fructose-1-phosphate by the enzyme fructokinase.
- Without the investment phase, fructose metabolism is less regulated and proceeds more rapidly (than the more regulated glucose metabolism)
- Insulin does not regulate Fructose like it does Glucose
- The Krebs cycle is also disrupted by Uric Acid , causing more production of fat
- Fatty acids are produced from Acetyl CoA
- In a later section we will see how central metabolism plays a role in numerous metabolic routes
- The liver is the primary site for fructose metabolism.
- This rapid conversion favors fat synthesis and can lead to insulin resistance and metabolic disorders. }
Fructose Metabolism and Uric Acid
In the picture above, recall that every intermediate molecule represented by the circles is regulated by enzymes.
Due to the rapid depletion of ATP due to fast Fructose metabolism,
- the enzyme AMP Deaminase (AMPD) is activated.
- By converting AMP to IMP, AMPD helps to conserve phosphate indirectly.
- Uric Acid is ultimately formed.
- Uric Acid causes Gout, disrupts the Krebs Cycle, and causes more Fat production.
- Notice that Uric Acid is a more oxygenated form of the purine section (nitrogenous base) of the AMP molecule.
- Here again we see how key nucleotides are in human biochemistry.
- AMPD then sends us down the pathway towards more Uric Acid and more fat storage and metabolic distress.
- Fascinating evolutionary theory:
- Evolution eliminated the enzyme Uricase from our bodies (other animals still have this).
- Uricase helps reject Uric Acid from our bodies.
- Fruit sources lessened as the climate cooled and
- Eventually we genetically adapted by eliminating Uricase.
- This allowed our human bodies to store more fat (via Uric Acid) in preparation for Winter.
AMPD is the Evil Twin of AMPK
- Recall that AMPK stands for AMP-activated protein kinase.
- Activated AMPK triggers the burning of stored fat while
- AMPD sends us down the path of fat storage.
- AMPD also triggers hunger by blocking the satiety hormone Leptin.
Fructose Forms
Just because fruits have Fructose doesn’t mean you need to stop eating fruits.
- Fructose enters our system relatively slowly when consumed from fruits
- In fruits, Fructose comes in mixed with fiber and Water.
- You’re not going to get fat eating fruit (well odds are , you’re not).
- Bigger risk comes from consuming concentrated sugar drinks including fruit juices
- where you are consuming a lot more fructose than you would via an apple for example
High Fructose Corn Syrup (HFCS) is a very widely used and cheap commodity. It is found in lots of processed foods.
- Most people believe this is a major contributor to modern metabolic dysfunctions
- Don’t let the name HFCS scare you off:
- HFCS is composed of 55% Fructose and 45% Glucose (Predominant in USA)
- Sucrose (Table Sugar) is 50% Fructose and 50% Glucose (Predominant in Europe but slowly changing)
- i.e. Fructose is found in all the regular standard sweeteners
- Fructose is being overconsumed today
{wymhacks: Uric Acid Measurement/Management}
High Uric Acid in the blood is bad (called Hyperuricemia when > ~ 7.2 mg/dl in blood per Medlineplus).
It Can cause Gout, increased fat, and metabolic dysfunction.
Foods that increase Uric Acid in the blood (Source: My.Clevelendclinic.org)
- Red meat.
- Organ meats like liver.
- Seafood (especially salmon, shrimp, lobster and sardines).
- Food and drinks with high fructose corn syrup.
- Alcohol (especially beer, including nonalcoholic beer).
Other good references:
- High Blood Uric Acid = 7.2 mg/dl (Medlineplus)
- Gout Low Purine Diet; My.Clevelendclinic.org
- How to Reduce Uric Acid: Healthline }
Monitoring /Biomarkers /Tests
Attia’s patients are monitored for various metabolism biomarkers
- Insulin
- Elevated Insulin – Canary in a coal mine of metabolic disorder
- Oral Glucose Tolerance Test (OGTT)
- Patient swallows ten oz. of a very sweet Glucola drink
- Rise and fall of insulin and glucose is then monitored
- Insulin rise/fall can be an early indicator of insulin resistance
- Blood Uric Acid
- Chronic Inflammation
- Elevated Homocysteine
- Elevated ALT liver enzymes
- Ratio of Triglycerides to HDL cholesterol (should be <2:1; target <1:1)
- VLDLs (Very Low Density Lipoproteins)
- HbA1c test; >=6.5% means Type-2 Diabetes
- Normal blood glucose is 100 mg/dL = Hemoglobin A1c (HbA1c) = 5.1%
- When blood glucose >=140 mg/dL (HbA1c >=6.5%) , ADA standard-of-care treatment guidelines kick in.
Insulin Resistance / Hyperinsulinemia
Attia sees preventing Metabolic Dysfunction as a cornerstone of his approach to longevity.
Studies have found that Insulin Resistance is associated with huge increases in the risk of
- Cancer (12x)
- Alzheimer’s (5x)
- Death from Cardiovascular Disease (6x)
Hyperinsulinemia is not really considered a bona fide endocrine disorder on its own.
Only after the advent of Type-2 Diabetes is any serious action taken.
So, since they play a major part in cancer, cardiovascular disease, and neurodegenerative disease, Metabolic Dysfunctions must be addressed first.
Part II. Chapter 7 – The Ticker
- Heart attacks are fatal roughly 1/3 of the time.
- Atherosclerotic Cardiovascular Disease (ASCVD)
- ASCVD = Heart Disease and Stroke (Cerebrovascular Disease )
- Leading cause of death in the US (more than cancer)
- Kills ~2300 people a day in the United States
- {wymhacks: See CDC for latest statistics (May 15,2024: 33 deaths per second)}
- American women are 10x more likely to die from ASCVD than from breast cancer.
- Attia mentored in this area by following experts
- Tom Dayspring
- Allan Sniderman
- Ron Krauss
- ASCVD is “relatively easy to delay if you’re smart and get on the case early”
- Classic Medicine 2.0 treats cardiovascular disease over an “overly short time horizon”
Vascular Network
Our Vascular Network comprises arteries, veins and capillaries.
{wymhacks: Let’s learn a little about these vessels (Source: Khanacademy.org):
Arteries
- Carry blood away from the heart.
- Typically carry oxygenated blood (except for the Pulmonary Artery).
- Have thick, muscular walls to withstand the pressure of blood pumped from the heart.
Veins
- Carry blood back to the heart.
- Typically carry deoxygenated blood (except for the Pulmonary Vein).
- Have thinner walls than arteries and often contain valves to prevent blood from flowing backward.
Capillaries
- Tiny blood vessels that connect arteries to veins.
- Have very thin walls to allow for the exchange of oxygen, nutrients, and waste products between the blood and tissues.
- Most of the body’s exchange of substances takes place in capillaries. }
If “stretched out and laid end to end”, we would have a 60,000 mile network of vessels. {wymhacks: ~2.5 x the earth’s circumference}
In addition to transporting 0xygen and nutrients to our tissues and carrying away waste, the Vascular Network also traffics Cholesterol between cells
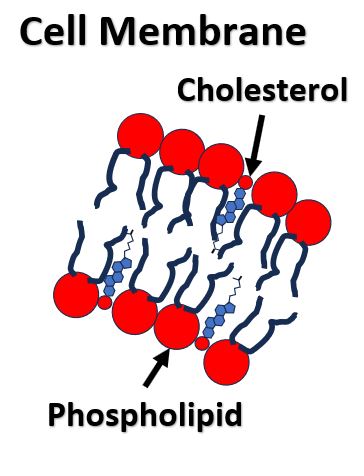
Cholesterol
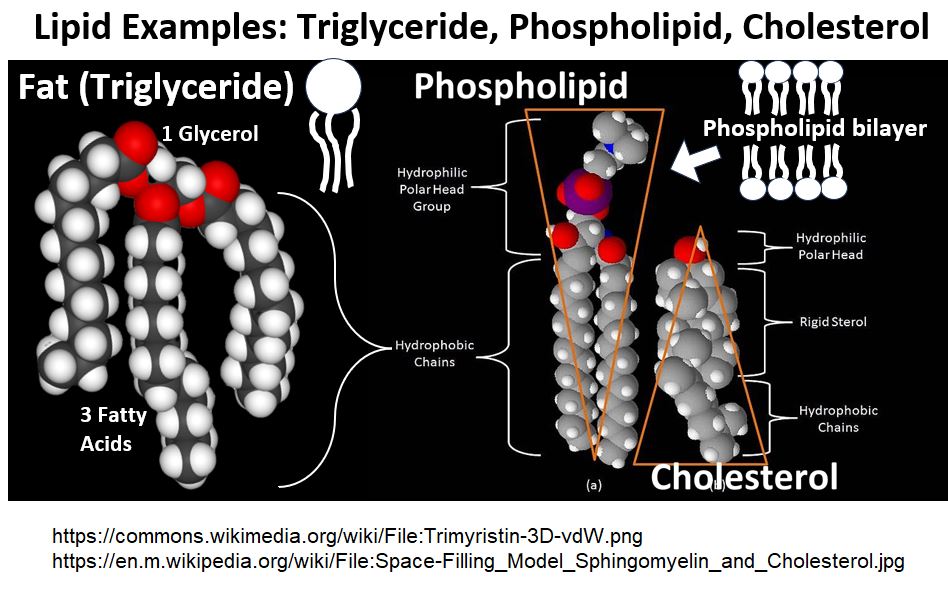
- cell membranes
- {wymhacks: Your body has roughly 30 Trillion Cells!
- According to this NCBI NIH article: “Cholesterol is the
- major sterol component of animal cell membranes,
- which makes up about 30% of the lipid bilayer on average.
- …Cholesterol plays pivotal roles in maintaining the structural integrity and regulating the fluidity of cell membranes” }
{wymhacks – Picture_Cell Membrane Cholesterol}
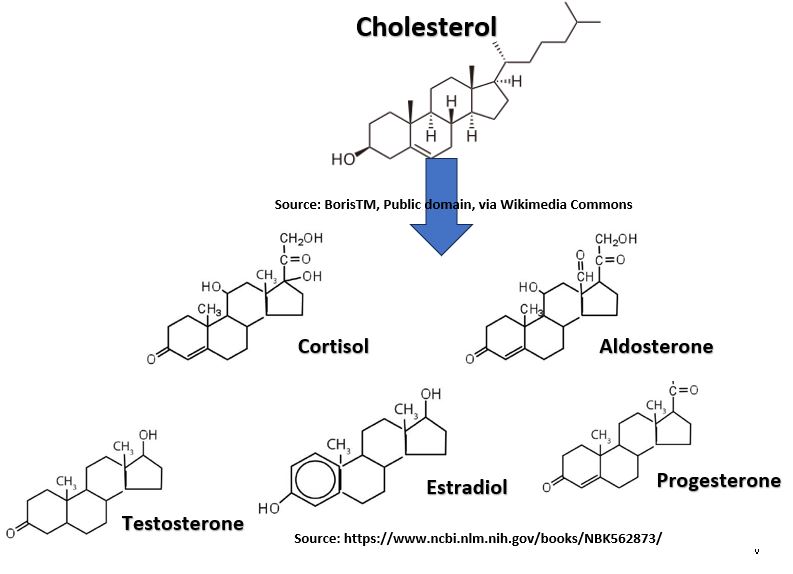
- Hormones (e.g. testosterone, progesterone, estrogen, cortisol, aldosterone)
{wymhacks – Picture_Examples of Cholesterol Derivatives}
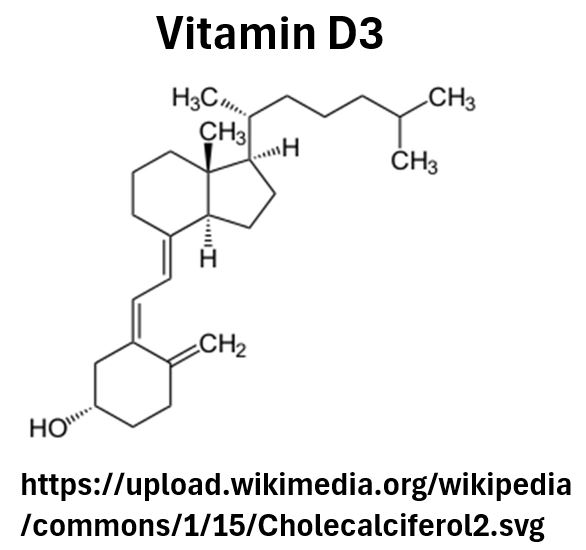
- Vitamin D
- {wymhacks: According to NIH.gov, “Type B UV (UVB) radiation with a wavelength of approximately 290–320 nanometers penetrates uncovered skin and converts cutaneous 7-dehydrocholesterol to Pre-Vitamin D3, which in turn becomes Vitamin D3”.}
- {wymhacks – Picture_Vitamin D3}
- Bile Acids (for food digestion)
All cells make Cholesterol but about 20% is stored in the liver.
- The Liver is a Cholesterol repository, distributing and receiving it.
Because Cholesterol is a Lipid (think fat), it’s not soluble in water or blood.
It therefore has to be carried around in spherical particles called Lipoproteins. {wymhacks: see my post Metabolic Pathways where I describe Lipoproteins called Chylomicrons}
Lipoproteins
Lipoproteins are
- little “cargo submarines” that move via the blood and
- distribute their lipid contents (Cholesterol, Phospholipids, and Triglycerides) to the body’s tissues.
- Lipoproteins can even transfer their cargos among each other.
See the generic picture of a lipoprotein below.
{wymhacks – Picture_Lipoprotein Structure}
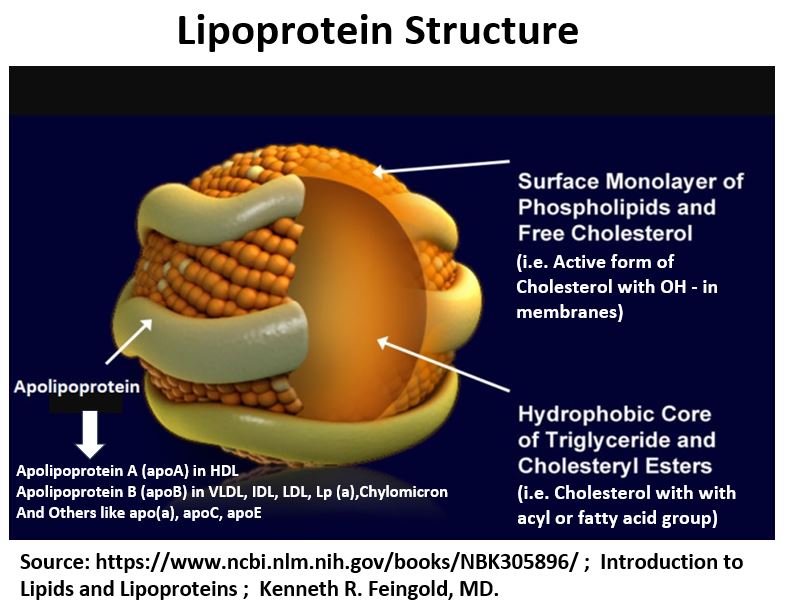
A lipoprotein consists of three parts:
- A lipid (cholesterol and other lipids) cargo on the inside.
- A surface monolayer that contains Phospholipids and “free Cholesterol”
- An outer non-continuous layer
- Called an Apolipoprotein.
- It wraps around the spherical structure.
- There are several types of Apolipoproteins.
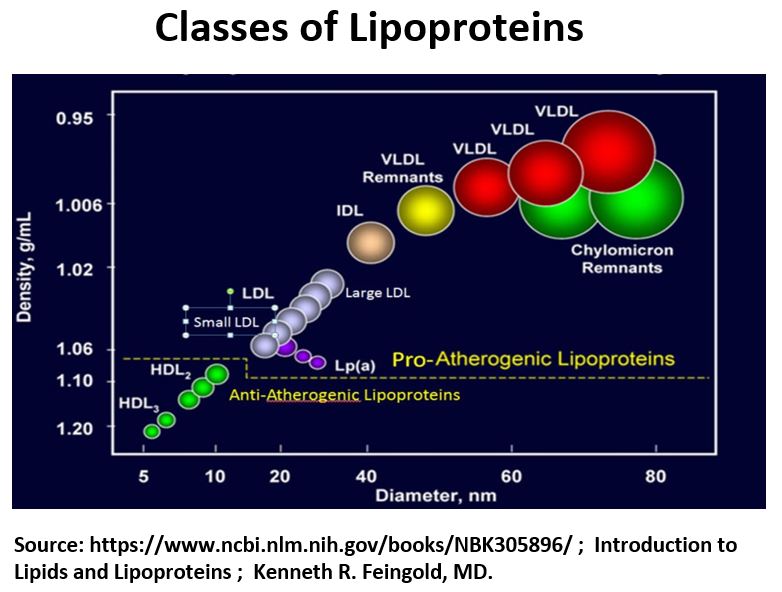
The Apolipoprotein type is the most critical differentiator among the different types of Lipoproteins.
- High Density Lipoproteins (HDLs)
- They are are more dense than other Lipoproteins, meaning
- they have more fat relative to protein.
- HDLs are wrapped with Apolipoprotein A or ApoA
- Low Density Lipoproteins (LDLs)
- are less dense than HDLs.
- are wrapped with Apolipoprotein B or ApoB
- There are other Lipoproteins (IDLs, VLDLs)
- IDL = Intermediate Density Lipoprotein
- VLDL = Very Low Density Lipoprotein
- These are also wrapped with Apolipoprotein B or ApoB
There are other types of Apolipoproteins , but it’s the ApoB that’s probably the most important.
LDLs, IDLs, and VLDLs contribute to Atherosclerosis and all carry this ApoB signature.
- LDLs, IDLs, VLDLs all contain ApoB
{wymhacks – Picture_Classes of Lipoproteins}
Our Current Understandings Dispel Some old Myths
- {wymhacks: According to this Harvard Article,
- your body manufactures most of its cholesterol with only about 20% coming in via food.”}
- Eating lots of saturated fats will increase bad lipoproteins but not true for cholesterol.
- Most of ingested cholesterol is excreted from out bodies.
- Eggs were vilified for years due to their cholesterol content, but since 2015,
- “the US Government Dietary Guidelines ” finally conceded that “cholesterol is not a nutrient of concern for overconsumption“”
- Cardiovascular disease does not only strike old people
- In men, 25% of cardiovascular events (heart attack, stroke, stent, graft) occur before age 54!
Atherosclerosis
Take a look at the two pictures below as you read this section.
{wymhacks: According the American Heart Association,
- “Atherosclerosis is a condition that develops when a substance called plaque builds up in the walls of the arteries.
- This buildup narrows the arteries, making it harder for blood to flow through.
- If a blood clot forms, it can block the blood flow. This can cause a heart attack or stroke.” }
{wymhacks: Blood vessels comprise three sections (we are oversimplifying quite a bit)
- The Artery Wall
- A thin layer covering the wall called the Endothelium
- The flow space which is called the Lumen
The Endothelium
- is a semipermeable barrier that controls the movement of molecules into and out of the blood.
- maintains our “electrolyte and fluid balance”
- expands and contracts the vessel based on blood flow (modulated by Nitric Oxide (NO)) }
{wymhacks – Picture_Atherosclerosis (Planar Arterial View)}
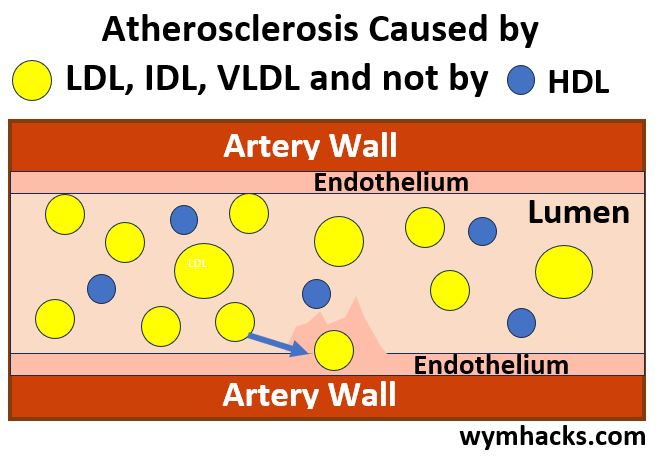
Endothelium Penetration
Lipoproteins, all kinds, will penetrate in and out of the endothelium (into the subendothelial space)
- but LDL particles will tend to stick.
- Other lipoproteins with ApoB will also stick (IDL, VLDL for example)
- These will react and be oxidized by reactive oxygen species (ROS).
- This causes oxidative stress (causing inflammation etc.)
- The accumulating ApoB laden lipoproteins begin to damage the Endothelium
A much better indicator of your exposure to risk from endothelial damage and ultimately Atherosclerosis
- is your ApoB count.
- ApoB is much more relevant than your cholesterol count.
Atherosclerosis Progression
Other heart disease risk factors like high blood pressure and smoking can also damage the Endothelium.
As the Subendothelial space starts getting engorged with ApoB particles (LDLs, IDLs, VLDLs, etc.)
- Immune cells called Monocytes are released and ultimately transform into
- Macrophages (“larger and hungrier immune cells”).
- Engorged Macrophages “blow up” into “foam cells“.
- Foam cell accumulation results in “fatty streaks“.
- Fatty streaks are precursors to Atherosclerotic Plaque.
- All of this begins developing in most of us at an early age.
HDL are considered “good lipoproteins” because they have “atheroprotective functions”
- HDLs sweep out excess lipids from the subendothelial space back into the bloodstream.
- New research suggests they maintain the structure of the Endothelium,
- lowering inflammation, and
- stopping the oxidation of LDL
- Measuring cholesterol content in LDLs (LDL-C) correlates well with heart disease risk,
- But knowing the concentration of LDL particles might be even more correlative
- Measuring cholesterol content in HDL (HDL-C) however, does not correlate well.
{wymhacks – Picture_Atherosclerosis (Cross Sectional Arterial View)}
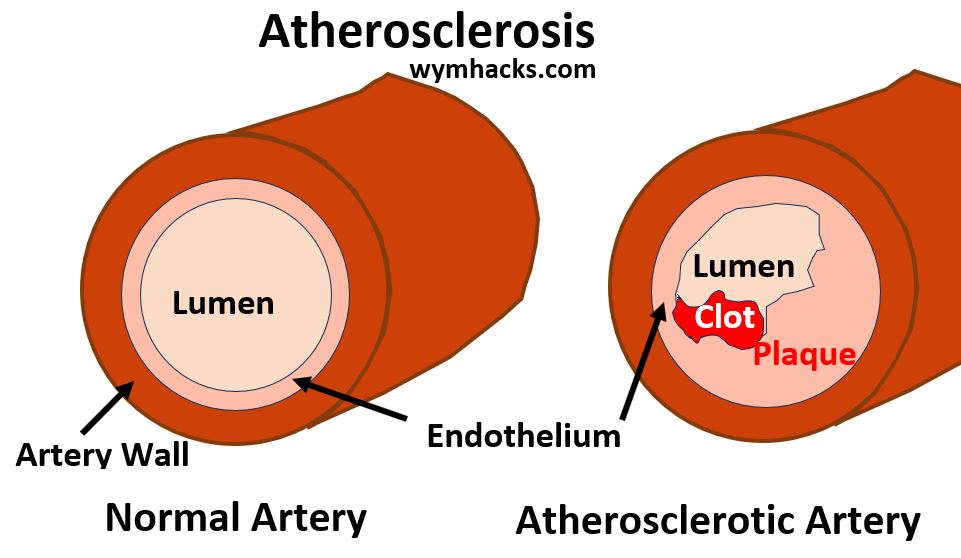
Atherosclerotic Plaque and Blood Clots
The growing plaque (accumulated foam) is eventually sealed from the arterial wall by a matrix barrier. It keeps growing though.
- It’s still not easily detectible (CT Angiogram might catch it)
- The plaque tends to grow towards walls but will eventually start squeezing the lumen passageway (called Stenosis).
- The Plaque begins to calcify. A regular calcium scan will detect this.
- Unstable Plaque can form blood clots, or worse, break free and cause a heart attach or a stroke.
- Normally the result is restricted/blocked veins/arteries which can lead to
- Ischemia (heart attach due to low blood flow) or
- Infarction (stoke due to no blood flow)
ApoB
Necessary (but not guaranteed) criteria for developing heart disease
- High ApoB
- LDL oxidation (modification) i.e. plaque and calcium
- High inflammation
The ApoB blood test is more predictive of cardiovascular disease than LDL-C
- More and more evidence to support this
- Attia: “I have all my patients tested for ApoB regularly…”
Lp(a)
Another lipoprotein called Lipoprotein (a) or Lp(a) is wrapped with a protein called Apolipoprotein a or Apo(a)
- Not to be confused with ApoA
- Apo(a) is stickier than ApoB
- Speeds the formation of Plaque
- If you have a family history of premature attacks, check your Lp(a) levels
How to Reduce Cardiovascular Risk
Attia mainly looks at ApoB and Lp(a) in his patients for indicators of cardiovascular risk.
ApoB also shows
- concentration of LDL particles
- concentration of VLDL particles
LDL-C as a proxy for ApoB
Treatment guidelines suggest
- 100 mg/dL LDL-C for patients at normal risk
- 70 mg/dL LDL-C for patients with high risk
Attia thinks these are too high:
- They should be much lower.
- See article by Peter Libby in Nature.
- 10 – 20 mg/dL LDL-C (levels we have when we were babies)
- these low levels don’t appear to be harmful
Attia Approach
- Smoking and high blood pressure damage the endothelium
- So, stop smoking !
- Control your blood pressure!
- Reduce ApoB, i.e. reduce LDLs and VLDLs via diet
- Consider lowering triglycerides
- Reduce saturated fats (shift to monounsaturated fats)
- Monitor other metabolic health indicators
- Insulin
- Visceral fat
- Homocystein (strongly correlated to increased risk of
- Heart attack
- Stroke
- Dementia
- HDL-C not that useful (HDL function seems more important but cant be tested)
- Reduce ApoB with Drugs
- Statins, lower LDL cholesterol levels by
- reducing the amount of LDL the liver produces and
- by helping the liver remove LDL from the bloodstream.
- Cannot be used by everyone due to side effects and specific conditions
- Prevention needs to start with people in their 30s and 40s!
- Read Sniderman et al article
- Look at a 30 year timeframe, not a 10 year timeframe
- Take aggressive precautionary measures early
References
Part II. Chapter 8 – The Runaway Cell
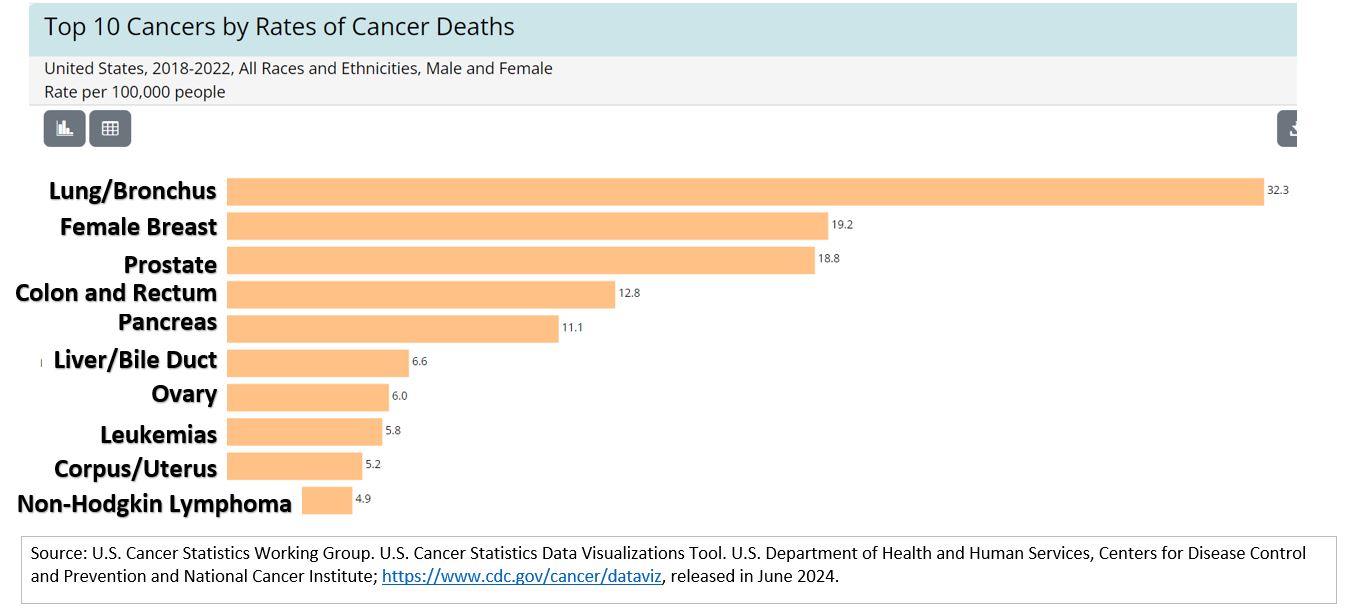
{wymhacks: Cancer Statistics}
- American Cancer Society Facts and Statistics
- Look at the latest annual report for some historical trends
- Over the last 10 years, most cancer rates have been flat (no change)
- Lung cancer rates since 1990 have dropped dramatically (not as many smokers)
- CDC Cancer Statistics at a Glance
Picture_Top 10 Cancers by Rate (USA, 2018-2022)
Outlive Chapter 8 Introductory Material
- The book “The Transformed Cell” by Steve Rosenberg influenced Attia’s decision to go into surgical oncology.
- Cancer is the second leading cause of death {wymhacks: In USA and Globally}
- Cancer is a disease of aging.
- It increase exponentially as one ages
- See the Parabolic graph at the National Cancer Institute
- Two problems with Cancer
- Not many effective treatments
- We can remove tumors but
- If Cancer spreads (metastasized), its very tough to treat
- Hard to detect cancer in early stages
- Not many effective treatments
- Three part strategy for dealing with Cancer
- Avoid getting cancer (we mostly don’t know how to do this)
- Use of newer, smarter treatments to target cancer characteristics
- Insatiable hunger for glucose
- Vulnerability to immune base therapies
- Detect cancer early
- early, aggressive and broad screening
- Colonoscopy at 40
- Pair these with Liquid Biopsies (detecting cancer via blood tests)
What is Cancer?
- Cancer cells don’t stop growing (they don’t grow faster than other cells, they just don’t stop growing)
- Gene Markers: e.g. Damaged Cell growth suppressor gene PTEN (often mutated or lost in people who have cancer)
- They can spread or metastasize
- Often turns a manageable disease into a deadly one
- The Cancer Genome Atlas
- Ambitious project started 20 years ago
- Couldn’t find much genetic similarity even for same cancer cases
- Cancer mechanisms are extremely complex
- Even if treated successfully, cant tell if cancer will come back or not
- Metastasis is still not understood and very little research goes into understanding it
- Once Metastasized cancer has to be treated systemically
- With chemotherapy (Chemo) typically.
- Chemo medicines are also poisons.
- Earliest chemo medicines were Mustard Gas derivatives.
- Hope is to selectively kill cancer cells.
- Metabolism and immune surveillance
- Two key cancer hallmarks discovered
- Cancers have altered metabolism (consume huge amounts of glucose)
- Cancers able to evade the immune system
- Potentially promising learnings and treatments might come out of these.
Cancer Metabolism
- 1920’s: Auto Warburg (Cancers love glucose)
- Cancer can consume 40x more glucose than normal cells, but
- they don’t respire normally (more anaerobically than aerobically) – even with plenty of oxygen
- Called the Warburg Effect (Anaerobic Glycolysis)
- Lew Cantley – Harvard – metabolic aspects of cancer
- Cancer fuels it proliferation via the Warburg Effect (less energy but lots of by product building blocks e.g. lactate)
- Also the acidic byproduct environment might prevent or slow immune cells from acting
- Obesity and Type 2 Diabetes fueling increased risks of cancer
- {wymhacks – cancer.gov – Obesity Associated with several types of cancer}
- Probably driven by inflammation and insulin.
- PI3 Kinases (PI3K) fuel Warburg Effect
- Cancer cells turn PI3K activity (speeds up glucose uptake)
- Cancer cells shut down PTEN (Cell growth suppressor gene)
- PI3K also turned up by Insulin and IGF-1 (insulin like growth factor)
- So Insulin acts as a kind of cancer enabler
- So, metabolic therapies (e.g. dietary adjustments) could lower insulin which could lower cancer risk
- Caloric restriction might have this effect of lowering insulin
- Bottom line: Avoid being anywhere on the spectrum of insulin resistance to Type 2 Diabetes because these elevate cancer risk
New Treatments
- New class of drugs, PI3K inhibitors, that fight cancer metabolism, don’t work as well as expected.
- They end up raising insulin
- Combined with a ketogenic diet , PI3K therapy might work better.
- Drug treatment combined with nutritional interventions are being actively explored.
- Concept/theory: Cancer cells are metabolically greedy so they might be more vulnerable to a reduction in nutrients (i.e. insulin).
- Stacking different therapies might be more effective (e.g. ketogenic diet + PI3K)
The Promise of Immunotherapy
- “The immune system is programmed to distinguish “non-self” from “self”
- It identifies pathogens and foreign bodies and attacks them
- Check out my post The Immune System – A Primer to learn more about B and T White Blood Cells.
- Immunotherapy is anything that trys to harness the immune system to combat an infection or other condition
- For cancer immunotherapy to work, immune system needs to recognize “bad self” from “good self.”
- Interluekin-2 (IL-2) – amplifies activity of lymphocytes (white blood cells). Marginally successful in cancer treatment.
- T-Cells are a type of white blood cell that play a central role identifying and destroying infected (or cancerous cells).
- Can take T-Cells, mark them with cancer cell antigens, and thus program them to attack those cancer cells.
- See the section titled “The Roll of T-Cells in Adaptive Cell Mediated Immune Responses” in the Immune System Primer.
- These T Cells are called Chimeric Antigen Receptor T Cells or CAR-T. (Approved for use by FDA in 2017)
- CAR-T only good against B-Cell Lymphoma.
- {wymhacks: T Cytotoxic Cells (see Immune System Primer for more information)}
Picture:T-Cytotoxic Cells (Tc Cells)
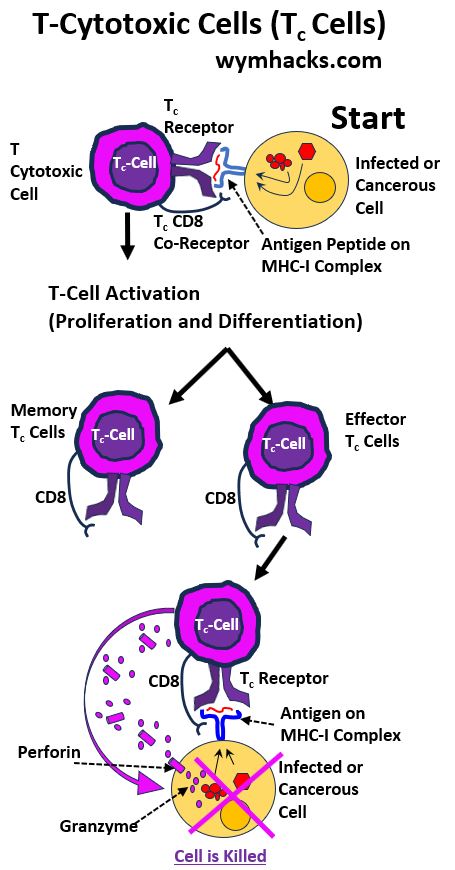
- Another treatment called “Checkpoint Inhibitors” make the cancer visible to the immune system.
- Checkpoints like CTLA-4 and PD-1 regulate and limit T Cells attacking our own cells.
- Inhibiting these allow the T Cells to see and attack cancer cells
- About 1/3 of cancers can be treated with immunotherapy and about 25% of those patients will benefit(so only 8.3% potential cancer deaths are prevented).
- Combining (Stacking) immunotherapies is being explored these days.
- Adaptive Cell Therapy – ACT – In this approach, a large amount of CAR-T cells are injected into the body to try to overwhelm the cancer.
- These developing therapies are very expensive at this time.
- Immunotherapy when it works seems to reduce the odds of remission compared to traditional treatments.
- There is Hope these will be more successful going forward.
Early Detection
- Early aggressive screening is most important prevention tool
- Too many cancers are detected too late
- 10 year survival rate with people who have metastatic cancer is 0 (same as it was 50 years ago)
- Cancer detection at Stage 1 mean your chances of survival skyrocket.
- Out of dozens of cancers only 5 have reliable screening methods
- lung
- breast
- prostate
- colorectal
- cervical
- Possible false positives make some people reluctant to test for cancer (cost issue)
- Diagnostic tests: tradeoff between Sensitivity and Specificity
- Sensitivity: ability of test to detect an existing condition
- Specificity: ability of test to determine someone does not have that condition
- Together, they represent test’s accuracy
- Must also consider prevalence of disease in our target population
- i.e. is this test being done on someone from a relatively low risk or high risk population?
Mammography: Sensitivity (mid 80s), Specificity (low 90s)
- If from low risk population (lets say 1% have cancer), your going to get a lot of false positives.
- In fact, “Positive Predictive Value” (PPV) of mammography is about 10% (i.e. if you test positive, there is only a 10% chance you actually have cancer).
- For a high risk population, the test has a higher PPV.
- Should stack tests to avoid misdiagnosis or improve “resolution” of diagnosis
- i.e. Use Ultrasound and/or MRI in addition to mammography
Prostate Cancer Screening
- This single test not enough to justify a very painful biopsy
- Must look at PSA Velocity, PSA Density, and Free PSA
- Could also do 4K blood test
- Doctor needs to answer: “Will our patient die with prostate cancer (as many men do) or will he die from it?”
- Can also use Multiparametric MRI imaging.
- Stacked together these tests avoid do unnecessary biopsies or surgeries.
Colorectal Cancer Screening
- Colonoscopy looks for tumors and polyps.
- “not all polyps become cancer but all colon cancers come from polyps”.
- Colonoscopy is excellent tool: does screening but also does surgery (can remove the polyps).
- There is some evidence that getting screened at 50 might be too late (even with patients with average risk factors).
- There are other screening tests (e.g. from stool samples) but Attia things “no other test compares to a colonoscopy”.
- 2018 American Cancer Society guidelines: get tested at 45 for people of average risk
- Attia recommends to get the test at age 40 (if you are above average risk – family history and certain medical conditions you might have).
- “Colon cancer has been documented to appear within the span of as little as 6 months to 2 years after a normal colonoscopy”
- For more guidelines and details see: peterattiamd.com – colorectal cancer screening
Scan Cancer and Melanomas
- Cancers are easy to spot visually
Cervical Cancer
- Pap smear: well established, minimally invasive
- Inside body cancers are tougher to screen
Can use low dose CT scans or MRI scans for Lung Cancer
- 15% of lung cancers occur to people who don’t smoke
- Lung Cancer is the #1 cause of cancer deaths
- MRI good to use also (less ionizing radiation than CTs)
- DWI MRI (diffusion weighted imaging with back ground subtraction)
- Imaging tests not perfect : have high sensitivity but low specificity
- Whole body MRI for example to screen for cancers might produce a lot of false positives
Liquid Biopsies (blood testing for cancers): Very promising
- As opposed to solid tissue biopsies
- Multicancer early detection – fast growing area
- Cancer cells tend to shed cellular matter including DNA
- Next generation high throughput DNA screening technology can detect these
A company called Grail (subsidiary of Illumina) offers the Galleri Test
- Trys to detect cancer and tell you where it is
- Has high specificity (99.5%) – i.e. telling you , you don’t have cancer.
- Sensitivity is low
- Still has much higher resolution than MRI or mammogram (imaging requires “seeing” the tumor)
- ? wym: its seems like its comparing apples to oranges when comparing sensitivities among different tests
- thelancet.com – GRAIL-Galleri: why the special treatment?
- healthline.com – The Galleri Blood Test for Multiple Cancers: What to Know
- Attia sees stacking (combining tests) as the solution (wym: well sure…when I used to trick or treat, I wanted to take all the candy but I couldn’t)
Chapter Concluding Remarks
- Of the Four Horsemen, cancer is the hardest to prevent.
- Aggressive screening is your best bet today.
- Only “modifiable” risks are
- smoking
- insulin resistance
- obesity
- pollution (maybe)
- “Treatment and prevention strategies are far less effective than tools available to address
- cardiovascular disease and
- the spectrum of metabolic dysfunction”
References
Part III – Chapter 12 – Training 101
- Need to work on cardio, strength, and stability
- cardio (continuum from walk to sprint)
- long steady endurance work – jogging , cycling, swimming (zone 2)
- max aerobic effort
- stability important – do the exercise using proper form and safely
Aerobic Efficiency – Zone 2
- zone 1 intensity: walk
- zone 2: going at an intensity slow enough to be able to maintain a conversation (but fast enough that it is strained)
- between easy and moderate
- zone 5,6,7: All out sprint
- “Healthy Mitochondria fostered by zone 2 training helps keeps fat accumulation in check”
- Mitochondria convert both glucose and fatty acids to energy (see my post: Metabolic Pathways)
- Glucose can be metabolized for energy outside (some of it via glycolysis) or inside (most of it via Krebs and ETC) the Mitochondria.
- Fatty Acids are converted to energy only in the Mitochondria.
{wymhacks – Picture Cellular Respiration in The Cell}
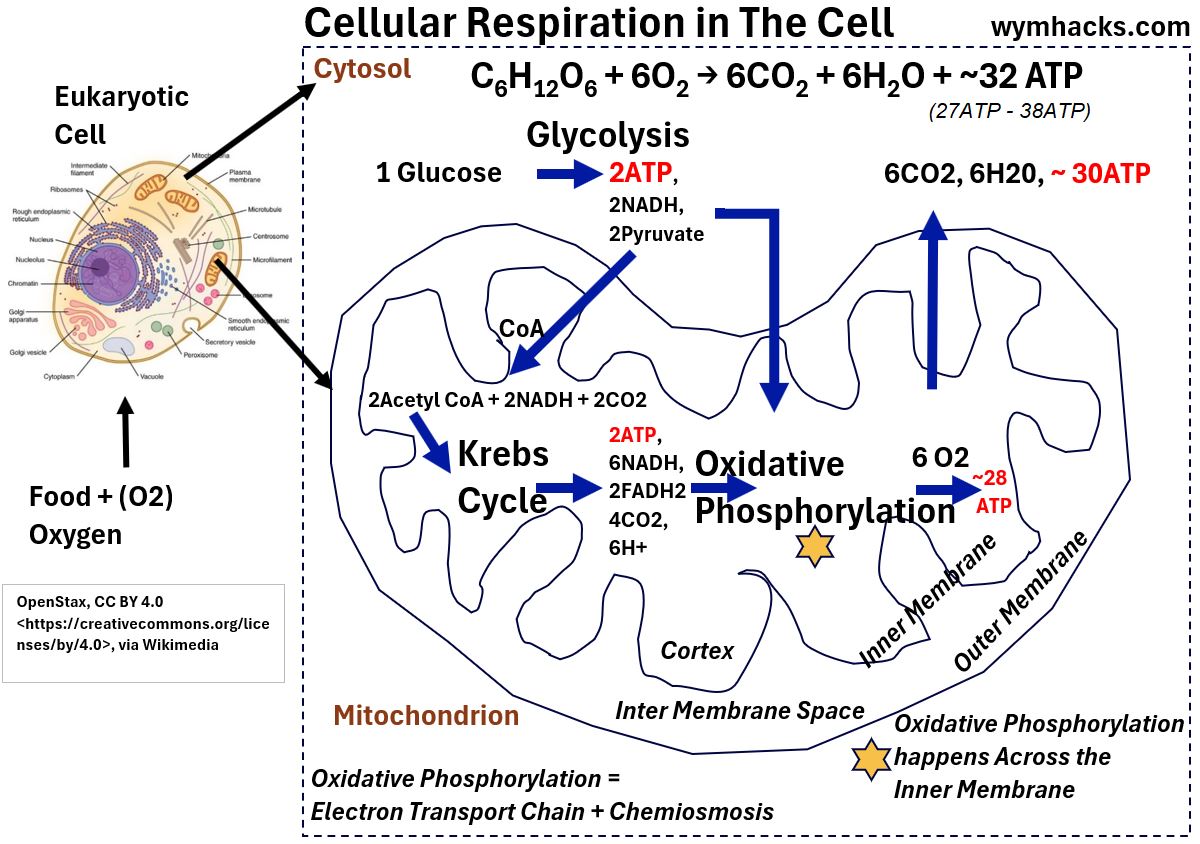
{wymhacks – Acetyl CoA in Central Metabolism}
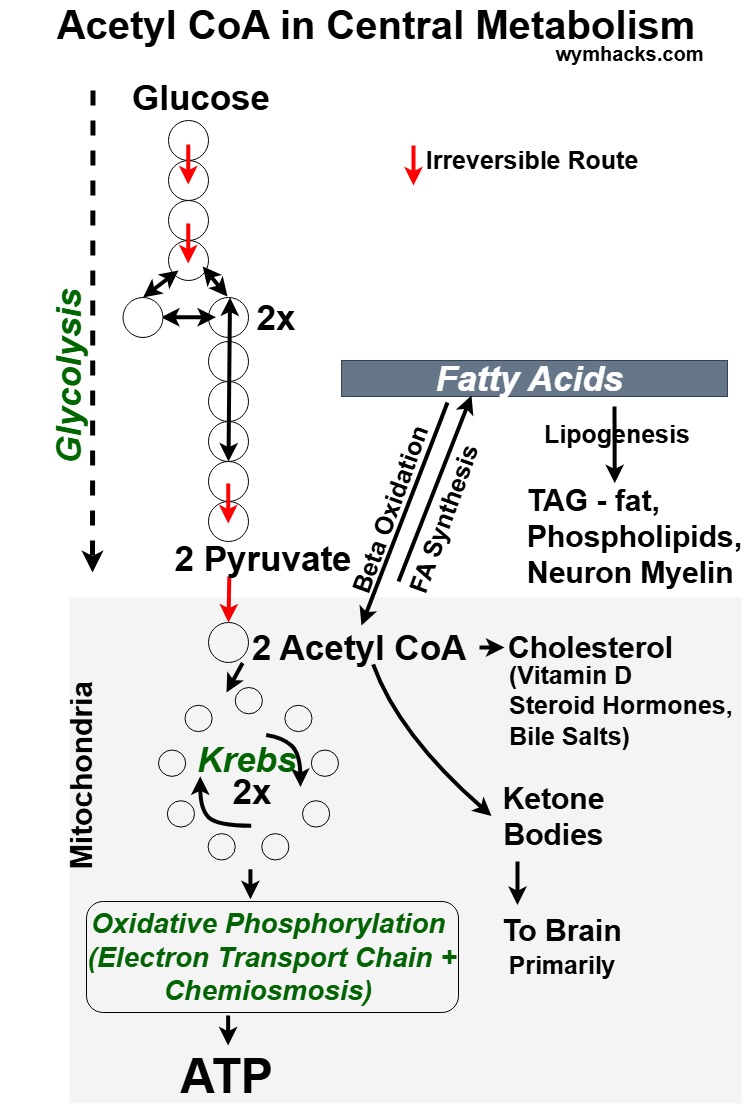
- Zone 2 training makes Mitochondria healthier allowing them to process fat more efficiently
- See this article by Barry Rotman, MD April 23, 2024
2017 Study by Brooks and Millan: Assessment of Metabolic Flexibility…
- Professional cyclist vs Sedentary individuals on stationary bikes
- Zone 2 endurance training is the key to keeping Mitochondria able to process fat efficiently
- Zone 2 workouts done by slow twitch muscles which have lots of Mitochondria
- Zone 2 is a max effort zone without accumulation of lactate.
- You shouldn’t “feel the burn” during a zone 2 workout
- You can measure your lactate with a lactate monitor(1.7 to 2 millimoles is a good range for Zone 2 workout says Attia)
- Zone 2 will be about 70 to 85% of your max heart rate (e.g. if max is 160, then zone 2 range is 112 – 136)
- Talk Test (Rate of Perceived Exertion) – can talk but not really carry on a conversation (i.e. you can uncomfortably converse)
- Zone 2 exercise produces healthier for metabolically flexible Mitochondria (can process glucose and fat efficiently)
- When we age, number and quality of our Mitochondria decline
Aerobic exercise creates new and more efficient Mitochondria. (Mitochondrial Biogenesis)
- Other “bad” mitochondria are recycled (mitophagy aka autophagy for mitochondria)
- Glucose uptake massively increases during exercise
- exercise triggers Non Insulin Mediated Glucose Uptake (NIMGU)
- can be effective in battling diabetes (body bypasses insulin resistance)
- Zone 2: ride a stationary bike, walk or jog , swim laps
- Check intensity – can talk in full sentences but just barely
- Zone 2: 3 hours per week (four 45 minute sessions) to derive a benefit
- Attia does 1 hour on stationary bike, 4x a week (at zone 2 threshold)
Measure your watts while you bike
- take average wattage for workout and divide by weight: e.g. 125 watts avg / 60 kg weight = 2 watts / kg
- 2 watts per kg for reasonably fit person
- 3 watts per kg for very fit person
- professional cyclist 4 and greater
- Zone 2 will produce more BDNF also (Brain Derived Neurotrophic Factor)
- Zone 2 workouts should be the foundation of your workouts
Maximum Aerobic Output: VO2 Max
- high intensity
- hard minutes long effort
- aerobic combined with anaerobic
- want to be at our max rate of O2 consumption
- you want to work on this once you have a good zone 2 workout foundation in place
- what is your VO2 max?. You should know.
- have to wear a mask. Pain in the ass. Painful.
- Age-related Decline In VO2max (Video by Jayson Gifford)
- VO2 max rapidly (steeply) declines with age
- and corresponds to a reduced functional capacity (to climb stairs etc.)
{wymhacks – VO2 Max Chart}
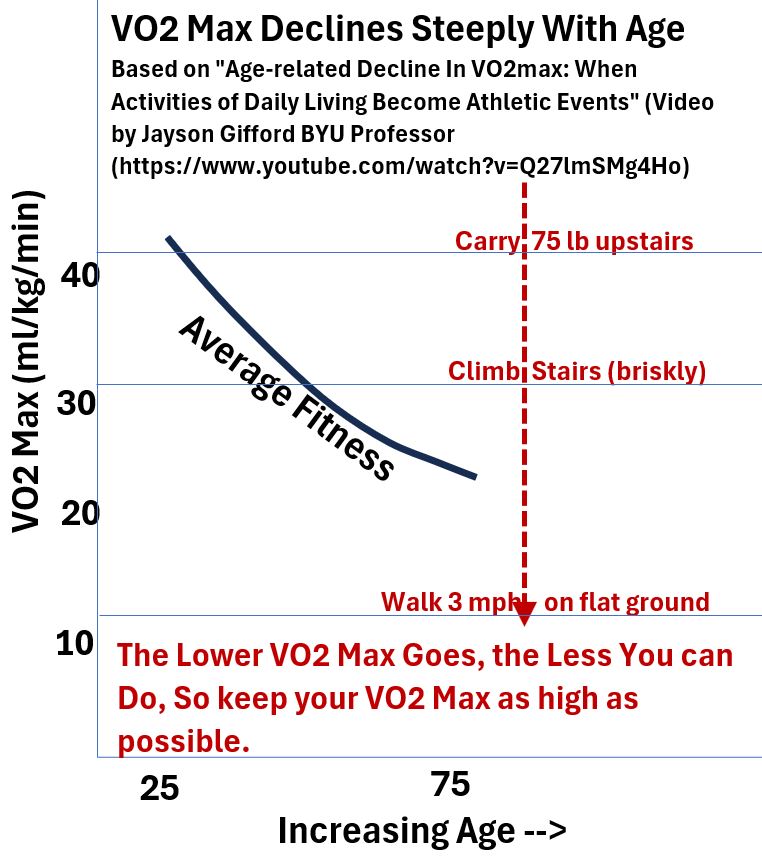
- Must keep you VO2 Max as high as possible so you can do basic functional stuff as you get older!
- VO2 Max will decline roughly 10% per decade (and more when you are over 50!)
- VO2 Max less than 18 ml/kg/min (for men; 15 for women) challenges your ability to live on your own.
- VO2 Max improvements will make you “functionally younger”.
- VO2 Max can “always by improved by training”
{wymhacks: Table – VO2 Max vs Age for Women and Men}
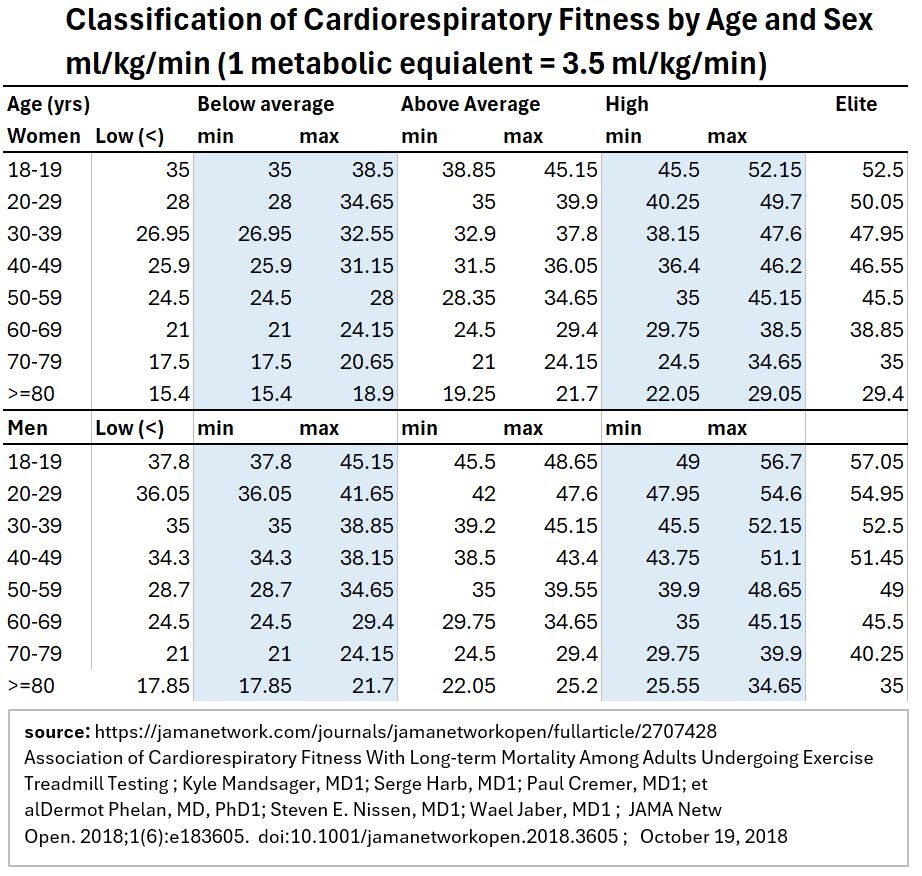
- Using table above. If you are a man in your 60s
- Lets say you are above average with VO2 Max of 29.75 (~30).
- If you increased this to 35, its now equivalent to an average person 10 years younger
- So, you want to do VO2 max work along with your Zone 2 workouts
VO2 Max workout recommendations
- Can do the workouts on a bike, rowing machine, or treadmill, or outside on a track
- warm up and cool down adequately
- Go 4 minutes at a maximum pace (that you can sustain)
- Then rest walk, jog easy for 4 minutes.
- Repeat four to six time
- For Attia: zone 2 is 150 watts, VO2 max training at about 200 watts
- A single workout a weak could suffice
- In the end you want to be :really good at going slow for a long time but to also
- be able to run hard and fast when needed”.
- You have to do this now to preserve your range of functions in later years.
Strength
- Muscle mass starts declining as early as our 30s.
- 80 year old will have about 40% less muscle than when he was 25.
- Per Andy Galpin, we lose muscle strength 2 to 3 x as fast as losing muscle mass
- We lose power (strength x speed) 2 to 3 x faster than we lose strength.
- Due to the “atrophy of our fast twitch type 2 muscle fibers”.
- Extreme Muscle loss: Sarcopenia. Indicator of Frailty.
- Frailty: when you meet 3 of these 5 criteria
- unintended weight loss
- exhaustion or low energy
- low physical activity
- slowness in waling
- weak grip strength
- Attia tracks Bone Mineral Density (BMD) – hips and lumbar spine (yearly in his patients)
- Using DEXA
- DEXA also measures body fat and lean mass
- Bone density “diminishes on a parallel trajectory to muscle mass”
- “1/3 of people over 65 who fracture their hip are dead within a year”
- Check your BMD every few years.
- Attia tests for BMD in middle aged persons. If there is a problem, possible options are:
- optimize nutrition (protein)
- implement heavy load bearing activity (stimulates bone growth and strength) – estrogen involved.
- Hormone Replacement Therapy (HRT)
- Drugs to increase BMD
- How much heavy things you can carry is important
- dumbbells, kettlebells, sandbags
- rucking – carry weight in a backpack or other strap on device (see Michael Easter)
Attia trains to improve the following
- Grip Strength
- Focus on both concentric (muscles shorten) and eccentric (muscles lengthen) loading (lift weight and put it back down)
- Pulling motions
- Hip hinging movements (deadlift and squat, step ups, hip thrusters, etc.
- Grip Strength
- Predicts how long your going to live
- Farmers Carry (carry dumbbells around) – keep shoulder blades down and back
- Dead hang from a pull up bar for as long as you can (you should be able to hang for 2 minutes)
- Concentric and Eccentric motion
- Concentric – Shorten (e.g. curl dumbbell to shoulder)
- Eccentric – Lengthen (e.g. extend dumbbell back to start)
- Step on and off an 19 inch block (with 3 second step down)
- Eccentric strength is where you typically need work
- For Eccentric, focus on the down phase of lifts
- Pulling
- Rows or pull ups
- Rowing machine
- Hip Hinging (bend at hips; not spine)
- Focus on Gluteus Maximus (Butt) and Hamstring
- start with single leg step ups (to begin)
- split stance Romanian Deadlift with no weight or light weight (to begin)
Part III – Chapter 15 – Putting Nutritional Biochemistry to Work
Standard American Diet (SAD)
The SAD environment is
- Plentiful
- Inexpensive
- Preserved
- Palatable
- Consumed in excess, the SAD harms us.
- Evolution has not prepared us for the plentiful calories from the SAD.
- Our bodies will readily become fat as glucose spills to fat
- Leading source of calories in SAD: grain based desserts (pie, cake etc.)
- SAD “wages war on our metabolic health”
- Almost all diets employ
- Caloric Restriction (most efficient)
- Dietary Restriction (most common)
- Time Restriction (intermittent fasting)
CR: Caloric Restriction – Calories Matter
- Too many calories end up as fat
- which can spill over into our organs, viscera, and muscle (See Chapter 6)
- Eating fewer calories lengthens lifespan (in lab animals)
- Monkey Studies (2009 U of W Madison, 2012 NIH)
- Eliminating junk food (avoiding diabetes etc.) helps longevity
- Strong link between Calories and Cancer
- Quality of Food is as important as quantity
- A high quality diet might mean a normal diet is sufficient (no caloric restriction) to maintain health.
- Limiting calories will help people who are metabolically unhealthy (and/or overnourished)
- Limiting caloric intake AND improving diet quality helps
DR: The Nutritional Biochemistry Diet
{wymhacks – See my post Macro Molecules, Minerals, and Vitamins; A Primer}
Alcohol
- 7 kcal/g (versus 9 kcal/g for fat and 4 kcal/g for protein and carbohydrates)
- Has zero nutritional value
- Ethanol oxidation Delays fat oxidation
- Causes mindless eating
- Ethanol is carcinogenic
- Chronic drinking associated with Alzheimer’s
- Metabolized in liver (bad for chronic drinkers)
- Attia: Limit to 7 servings/week, no more than 2 a day
Carbohydrates
- Carbohydrates digested to Glucose then converted to ATP
- Extra glucose in muscles and liver as glycogen or in adipose tissue as fat
- Insulin secreted when glucose in blood increases (to bring it back down)
- Excess calories can cause NAFLD to insulin resistance to type 2 Diabetes (see Chapter 6)
- Repeated blood glucose spikes could be bad in themselves
- Correlated to longevity (mortality)
- Different in each person (key point)
- Continuous Glucose Monitoring (CGM) – device that tracks blood glucose levels
- More accurate than HbA1c blood test
- Available only by prescription (?)
- Useful to track your food and see which ones spike your glucose
- Goal: lower average blood glucose level and reduce variability
- Target: keep average glucose <= 100 mg/dl (milligrams per deciliter) with a standard deviation of 15
- 100 mg/d = HbA1c of 5.1% (pretty low)
- Influenced by level of activity and sleep
- Stress elevates Cortisol, causes liver to secrete glucose into blood
- Attia will also test and track patients for weight, body composition (lean mass and fat mass)
- Attia will also track biomarkers like lipids, uric acid, insulin and liver enzymes.
Lessons from Continuous Glucose Monitoring
- Glucose spike higher/faster for more refined Carbs.
- Bread with fiber blunts the spikes
- Rice and Oatmeal with cause Glucose Spikes (including brown rice)
- Fructose not measured by CGM
- Aerobic exercise best for removing glucose from blood
- High intensity exercise and weight training tends to spike glucose (liver squirts glucose to feed the muscles). Attia says don’t worry about these spikes (why?)
- Sleeping less will spike your glucose more (5 or 6 hours versus 8)
- Stress via cortisol (especially during sleep) can spike glucose.
- Non-starchy veggies like spinach and broccoli wont spike glucose
- High protein and high fat food wont spike glucose
- Large amounts of lean protein will (chicken) slightly spike glucose
- Protein shakes might spike your glucose depending on what’s in them (i.e. low in fat and with sugar)
- Stacking of these things will make it worse
- Tracking glucose might improve our eating behavior due to Hawthorne Effect (you behave because you are being watched so to say).
Protein
- Protein (Amino Acids) are the building blocks of life (need for muscle and structure).
- As we age we lose muscle faster.
- Not a primary source of energy and isn’t stored like fat
- Excess is excreted in urine (urea).
- 20 amino acids are the building blocks for muscle, enzymes, hormones.
- makes up Hair, Skin, Nails, immune system molecules, etc.
- 9 (Essential) amino acids must be ingested via food because our bodies don’t make them.
- Attia: Recommended Daily Allowance = .8 g/kg body weight is too low.
- In the elderly, low protein = low muscle mass = greater mortality = worse quality of life
- Attia: 1.6 to 2.2 g/kg body weight should be protein target.
- For active people with normal kidney function target might be 1 gram/lb weight (2.2 g/kg)
- So if you weigh 150 lb, that’s 150 g of protein (that is a lot of protein to eat)
- Ideally consume it in 4 servings a day.
- Attia’s: Why protein shake + high protein snack + two protein meals
- Plant Protein: 60 – 70 % utilized by your body (see Don Layman)
- Plant Protein has less essential amino acids (methionine, lysine, tryptophan)
- So overall quality of protein from plants is significantly lower than from animal protein.
- Layman – Leucine and Lycine (3 – 4 g/d); Methionine (at least 1 g/day)
- Need more Leucine if you are building up muscle mass (2-3 g, four times a day)
- Healthy Aging and Body Composition Study
- Protein might improve insulin sensitivity and glucose control.
- Protein helps us feel satiated, inhibiting the release of hunger inducing hormone ghrelin (we then eat few calories).
Fat
- They are efficient fuel for oxidation (slow burning logs)
- Building blocks for hormones (through cholesterol) and cell membranes
- Important for health of brain (most of which is made up of fatty acids).
- Saturated Fats (SFA)
- saturated with hydrogen (more hydrogen)
- Monounsaturated Fats (MUFA),
- Polyunsaturated Fats (PUFA),
- Omega-6
- Omega-3 – Marine Sources (EPA, DHA) – Seafood
- Omega -3 – Non Marine Sources (ALA) – Nuts, flaxseed
- Trans Fats (largely removed from diets)
- Fatty Foods always have mixtures of SFA, MUFA, PUFA
- Attia for his patients:
- target 50%-55% of fat as MUFA;
- 15-20% as SFA;
- Remaining is PUFA
- Try to boost EPA, DHA (for brain and cardiovascular health)
- Test for EPA , DHA in membranes of red blood cells (specialized blood test)
- Like to see 8 – 12% of RBC membrane composed of EPA and DHA
- Attia patients
- eating more olive oil, avocados, nuts
- reducing omega-6 rich corn, soybean, sunflower oils
- increase high omega-3 marine PUFAs
- Studies on fats don’t overwhelmingly correlate superiority of one over the other but in general
- MUFA is best , then PUFA, then SFA
- Attia uses “expanded lipid panels” with his patients to track fatty acid consumption and cholesterol and “overall lipid and inflammatory response”
- {wymhacks – Standard Lipid Panel –
- measures total cholesterol,
- LDL cholesterol,
- high-density lipoprotein (HDL) cholesterol and
- triglycerides.}
- {wymhacks – Two commonly used advanced lipid tests are
- apolipoprotein B (ApoB; See Chapter 7) and
- LDL particle number (LDL-P).}
TR: The Case for (and Against) Fasting
- Fasting or Time Restricted (TR) eating
- Some good things happen when we are not eating
- Insulin drops
- liver starts depleting fats {wymhacks: 24 hours?}
- Within 3 days, starvation ketosis – fat used, ketones produced
- Longer term , mTOR turned down (see Chapter 5)
- Autophagy accelerated (cellular recycling process)
- Activates FOXO (cellular repair genes that may be helping Centenarians live so long) – See Chapter 4
- Scientific Literature on the topic is still weak
Short Term Fasting
- Eat food in a 6 or 8 hour window
- Probably need a tighter window
- Probably need 6 or 4 window
- Mice studies probably not valid
- Human trials don’t find much of a benefit
- Meeting protein targets will be difficult
- Maybe beneficial in reducing snacking (which Japanese call lonely mouth)
Alternate Day Fasting (ADF)
- Studies and tests not that conclusive
- Might lose muscle and your activity is reduced
- Attia: neither necessary nor wise
- Need to eat enough to maintain muscle mass and remain sufficiently active
- Attia uses fasting for extreme cases where there are few other options
- e.g. Patient Tom Dayspring
- One week per month severe caloric reduction diet
Conclusion
- Diet and Nutrition is important but is not the strongest lever for longevity
- “Bad nutrition can hurt us more than good nutrition can help us”
- Must balance caloric intake with meeting your Protein needs.
- Zone 2 Aerobic (long, steady type) enhance body’s ability to utilize glucose and fat
- Avoid fructose sweetened drinks (sodas and fruit juices) – Safe way to get fructose is directly from fruits.
- Diet plan improves or maintains
- blood glucose and insulin
- muscle mass
- lipid level
- weight
- Your diet depends on your risk profile for
- metabolic dysfunction – e.g. excess carbs leading to elevated triglycerides
- cardiovascular disease – e.g. lipoprotein issues
- Attia suggests (in general) that staying active and working out should be your main effort.
- Use your diet as an additional supporting weapon to improve your lifespan and healthspan.
Part III – Chapter 16 – The Awakening
- Many studies show getting less than 7 hours a night is powerfully associated with bad health outcomes
- get common cold easier
- dying of a heart attach
- increased metabolic dysfunction up to Type 2 Diabetes
- upsets hormonal balance
- affects our cognitive functions, memories, and emotions
- While sleeping , your brain dreams and even cleans itself (similar to people sweeping city streets)
- Sleep preserves our cognition as we age and perhaps staves off Alzheimer’s Disease.
- See Mathew Walker podcasts with Attia and read his book Why We Sleep.
- “Why would evolution allow us to spend up to a third of our lives in a state of unconsciousness?”
- “Sleep is as fundamental to our health as stability is fundamental to strength”.
- Many studies: Need to Sleep 7.5 to 8.5 hours a night.
- Affects our physical and cognitive performance (even one bad night).
- Lack of sleep increases odds of injury.
- Lack of sleep affects ability to drive.
- Danger is your body and mind can adapt to less (at its own peril).
Old Man Blood
- Navy Seals bloods tests showed hormone levels and inflammatory markers more common in much older men.
- Poor sleep “wreaks havoc on our metabolism”.
- Multiple studies: Poor sleep can cause major insulin resistance.
- Eve van Cauter – Sleep Scientist
- Inadequate sleep can “tilt” us towards Metabolic Dysfunction.
- Linked to Type 2 Diabetes
- Longer than recommended sleep can also be bad.
- 11 or more hours of sleep might increase risk of all cause mortality.
- Stress has something to do with this.
- Higher Stress can make us sleep poorly but also vice versa.
- Poor Sleep; High Stress: Both activate the Sympathetic Nervous System (SNS).
- Fight or Flight response
- Releases Glucocorticoids including Cortisol.
Cortisol
- Raises blood pressure.
- Causes liver to release glucose.
- Inhibits uptake / utilization of glucose by muscles and fat.
- High overnight glucose on a CGM (continuous Glucose Monitor) usually means high Cortisol.
Food
- Lack of Sleep (4 to 5 hours) reduces Leptin levels.
- Leptin hormone signals to us that we are fed.
- Lack of Sleep increases Ghrelin (hunger hormone).
- {wymhacks: Mnemonic – Leptin Lowers Hunger, Ghrelin Gains Hunger}
- Coming off of a poor sleep causes you to be excessively hungry.
- Lots of time people get this through junk food.
- Perfect recipe for NAFLD and Insulin Resistance.
Sleep and Cardiovascular Disease
- Sympathetic Nervous System (SNS)
- Threat Perception causes
- Cortisol secretion
- Adrenaline secretion
- Raise heart rate
- Raise blood pressure
- Lack of Sleep activates the SNS
- Can cause higher heart rates and increases irregularities
- So increased risk of heart attacks
- Two studies: < 6 hr sleep associated (tougher to prove causality) with 6 to 26% increase in cardiovascular disease.
- Study: < 6 hr sleep = 20% increase in risk of heart attack and sleeping 6 – 9 hrs reduced risk of heart attack.
Sleep and the Brain
- Sleep important for cognitive function and long term cognitive health.
- Some research: Chronic bad sleep causes Alzheimer’s Disease and Dementia.
- When we Sleep
- Heart rate slows down
- Core temperature drops
- Breathing becomes regular
Sleep Stages (analogy of a submarine)
{wymhacks – Hypnogram – Sleep Stages – Normal Healthy Adult}
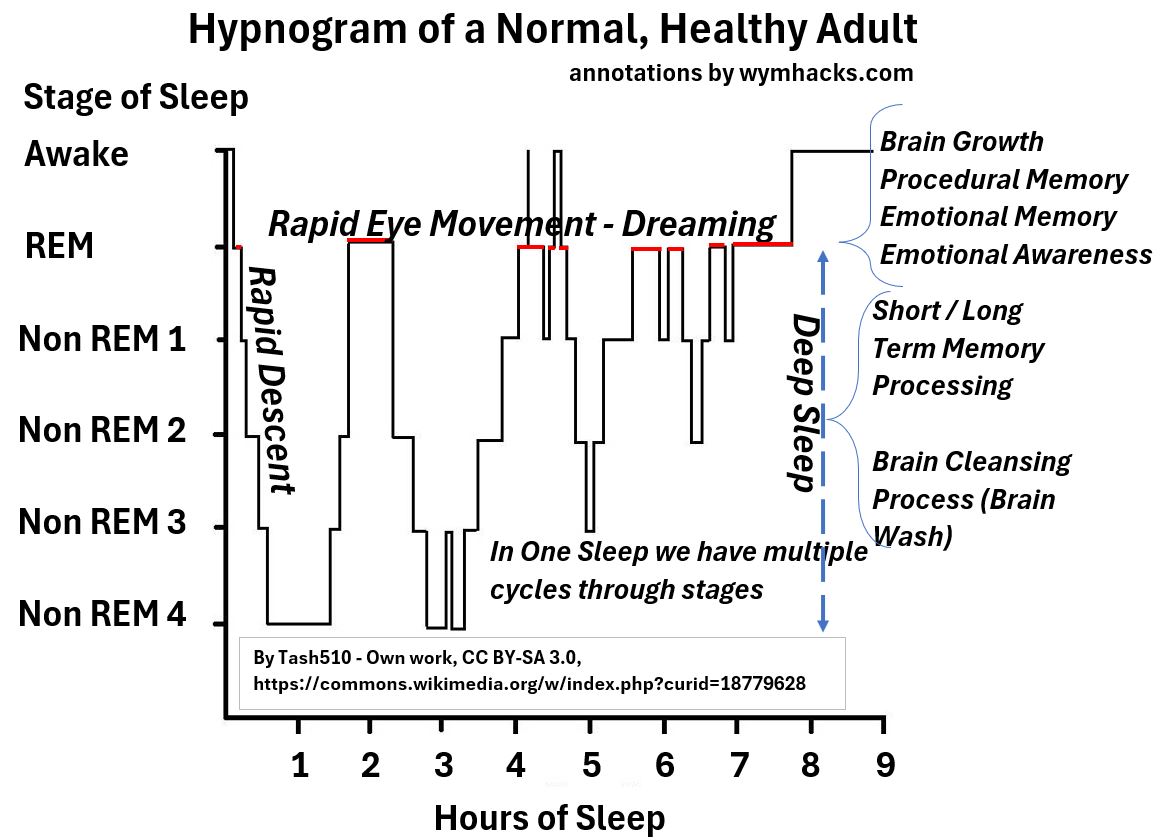
- Initial Sleep (submarine slips beneath the waves)
- Rapid descent to Deep Sleep.
- Deep Sleep: Non-REM or NREM (Non Rapid Eye Movement) sleep
- Two substages: Light NREM and Deep NREM
- Cycle between these
- Deep NREM: Brain waves slow, reaching a very low frequency (1-4 cycles per second)
- Dominates the first 1/2 of the night.
- REM Sleep: Eyeballs dart around as we dream.
- Electrical signature of REM sleep is similar to when we are awake.
- Difference is our bodies are paralyzed.
- {wymhacks: Ever had one of those can’t get up or can’t escape dreams?}
Deep Sleep
- Short term memories in Hippocampus cleared out or stored in Cortex.
- Getting a good sleep is correlated with doing better on memory tests.
- Keeps our brain healthy
- Cerebrospinal fluid into neuron areas that sweeps away “intercellular junk”.
- Deep Sleep washes the brain (e.g. the Amyloid Betas and Taus – linked to neurodegeneration – See Chapter 9)
- Studies: Chronic under sleep (<7 hrs) results in buildup of Amyloid Beta and Tau.
REM Sleep
- In youth, helps brain grow and develop
- Developing neural networks
- Plateaus in Adults but important for creativity and problem solving
- Good for procedural memory (e.g. new ways of moving body)
- Emotional memories are processed (always feel better in the morning)
- So helps with controlling anxiety
- Helps us maintain emotional awareness
- Up to 1/2 people with Alzheimer’s Disease have Sleep Apnea.
- “Sleep disturbances may create conditions that allow Alzheimer’s to progress.”
- “Superior sleep quality in older adults associated with a lower risk of developing MCI (Mild Cognitive Impairment) and Alzheimer’s. “
- Irregular or fragmented sleep is bad for the brain
- Ability to get deep sleep declines with age .
- Possibly related to growth hormone secretion changes
- Good sleep in middle age (40s to 60s) seems to be important for “maintaining cognitive health”.
Assessing Your Sleep
- Morphine puts people to sleep (bad for other reasons, addictive, etc.)
- Ambien (zolpidem) and Lunesta do not promote healthy long lasting sleep.
- Orexin Antagonist Inhibitors (Dayvigo and Quviviq) – promising but expensive medicines for insomnia
- Benzodiazepine Drugs (Valium, Xanax – sometimes used to treat insomnia) – typically don’t improve sleep quality.
- Trazodone – anti-depressant – helpful for sleep and quality
- Ashwagandha – helps with sleep quality also
- No drug magic bullet today for sleep
Things to do to improve sleep
- Admit you need more sleep
- Assess your sleep
- Use Sleep Tracker (monitors heat rate, heart rate variability, movement, breathing rate, and more)
- Do the Pittsburg Sleep Quality Index questionnaire.
- Or do the Epworth Sleepiness Scale quiz (see this CDC site)
- Or do the Insomnia Severity Index
- Know your Sleep Chronotype (are you a morning person or not?)
- Morning person will have different circadian genes
- To determine Sleep Chronotype take the Morningness / Eveningness Questionnaire (MEQ)
- Adolescents tend to wake up later (should school times be adjusted later?)
- Do you have Sleep Apnea? (Take STOP-BANG Questionnaire) – it’s a serious medical problem.
Sleeping Better
You obviously will have to address your Sleep Apnea or other specific problem more specifically, but here are some things you can do to improve your sleeping.
- Create Environment conducive to sleeping (darkness)
- Turn off all your shit (no lights)
- Non natural lighting blocks release of melatonin. (darkness activated hormone that helps with sleep)
- Similar to way that SAD (Standard American Diet) interferes with satiety hormones
- Don’t stare at your devices before you go to bed (at least an hour before bedtime)
- Keep the bedroom cool (65 F is optimal…{wymhacks: really?})
- Cut back on Alcohol (not good for REM sleep; affects your memory)
- Coffee – inhibits receptor for adenosine (helps us go to sleep)
- 1/2 life (concentration drops by 1/2) of Coffee is 6 hours
- We need to cultivate Sleep Pressure (our need or desire for sleep)
- Napping counteracts this
- Exercise helps with Sleep Pressure (especially Zone 2 endurance exercise)
- Exercise with exposure to sunlight (1/2 hour dose of strong daylight helps keep our circadian cycle on track
- Mentally prepare yourself for sleep (avoid stressful things – turn down Sympathetic Nervous System)
- Meditate
How to Improve Your Sleep List
- No alcohol (or one drink before 6 pm)
- Dont eat inside 3 hours
- No stimulating electronics (inside 2 hours)
- No anxiety producing work (inside 2 hours)
- Spend time in Sauna or Hot tube before bed
- Cool room (mid 60s F) – use cool mattress
- Darken room completely – use eye shade if necessary
- Fix your wake up time – dont deviate much from it
- Target 8 hours of sleep
- Don’t obsess over your sleep
- If you still can’t Sleep
- Stop fighting it. Get up. Drink non caf tea and read a boring book.
- Key is find something relaxing and enjoyable but serves no function
- Check your chronotype (are you a night owl?). Adjust your sleeping.
- If Sleeplessness Persists
- Do Cognitive Behavioral Therapy for Insomnia CBT-I.
Attia considers sleep a “performance enhancing substance” for physical and cognitive health.
Your Evolution has required it so optimize it for a longer lifespan and healthspan.
Part III – Chapter 17 – Work in Progress
- “Emotional health and physical health are closely intertwined”
- Suicide obviously impacts lifespan
- Suicide among top 10 cause of death among all age groups
- CDC: >100,000 Americans (April 2020 to April 2021) died from drug overdoes (as much as from Diabetes)
- Drug overdoses account for 40% of accidental deaths
- Emotional Health: Maybe the most important component of healthspan
- Without happiness, fulfillment, connection to others, its not worth it
- Living alone or being lonely is linked to much higher risk of mortality.
Trauma categories
- Abuse
- Neglect
- Abandonment
- Enmeshment (blurring of boundaries between adult and children)
- Witnessing tragic events
- Most therapists diagnose people using The DSM
- Diagnostic and Statistical Manual of Mental Disorders
- Can always find a tidy diagnosis
- See Podcast with Paul Conti
- Hard to give blanket advice
- Problem with Medicine 2.0 today
- Diagnose
- Prescribe
- Bill
- Mental health and emotional health are not the same thing
- Mental Health – Disease like states (clinical depression, schizophrenia)
Emotional Health – Much broader including how to manage emotions and interpersonal relationships
- We should address Emotional Health earlier on
- Must be proactive
- Hard to recognize signs that you might need that Emotional help
- Book: “I don’t want to talk about it” – By Terrence Real – Roots of male depression
- Consider therapy
- “90% of male rage is helplessness masquerading as frustration”.
- think of relationships as a “delicate ecosystem”
Attia corrections
- spend time with kids
- check in with wife on her stuff
- reframe things: look at a situation from someone else’s point of view
- and why is your situation more important than theirs
- David Foster Wallace commencement class speech (Kenyon, 2005)
- Power of Reframing
- “Step back, temper your reflexive actions, try to see what is actually happening. “
- David Brooks: The Road to Character
- Resume Virtues – your living CV
- Eulogy Virtues – what people say about you when you die (focus on these)
- Who cares how well you do if you are miserable all the time?
- PCS – Psychological Counseling Services – Phoenix Arizona
- Listing Affirmations is helpful (one positive affirmation for each year of your life)
- Jacob Riis:
- “When nothing seems to help, I go back and look at a stonecutter hammering away at his rock perhaps a hundred times without as much as a crack showing in it. Yet at the hundred and first blow it will split in two and I know it was not the last blow that did, but all that had gone before.”
- “True recovery required probing the depths of what shaped you, how you adapted to it, and how those adaptations are now serving you” (or not)
- Be proactive. Look for problems early.
Dialectical Behavior Therapy (DBT)
- Marsha Linehan
- Cognitive Behavioral Therapy Principles
- Clinical trials show it helps prevents suicide and self harm
- Skills based;
- Specific Skills,
- Practiced repeatedly
- Under stress.
- Break chain of Negative (-) Stimulus to (-) Emotion to (-) Thought to (-) Action
- Mindful approach to deal with
- Emotional Regulation,
- Distress Tolerance,
- Interpersonal Effectiveness,
- Self Management.
- For DBT Distress Tolerance Attia
- Many of the practices discussed in the book help to maintain and widen this
- Mindfulness helps with Reframing.
- Create a gap between stimulus and response to avoid acting reflexively.
- Suffering often not due to direct cause (more like past or future event).
- Seneca: “We suffer more often in imagination than in reality.”
- Listen to your self talk.
- DBT Emotion Regulation
- {wymhacks – Have to dig deep and understand the real cause in order to control and regulate it.}
- DBT Distress Tolerance
- Use counter acting techniques that stimulate the Cranial Vagus Nerve.
{wymhacks – Vegus Nerve}
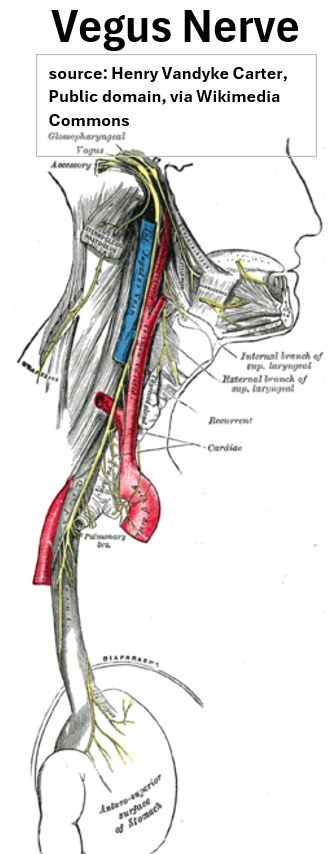
- Vagus Nerve controls heart rate and respiratory rate in or out of Parasympathetic (calm) or Sympathetic Mode (fight or flight) .
- Ice water in face or take cold shower,
- Slow Deep Breathing (4 second inhale, 6 second exhale),
- {wymhacks – Based on link above – exercise regularly, Massage yourself (e.g. feet), Listen or Create Music}
- Attia Rucks (walking with weighted vest or backpack) to help with emotional health.
- DBT Opposite Action
- Do reverse of something bad that you are about to do
- “Changing the behavior can change the mood“.
- Attia says that regular therapy is probably his most important tactic of all.
Concluding Remarks
To fix Emotional Issues, you have to first believe that you can change.
Believe that It’s ok to be vulnerable and to ask for help.
Paulo Coelho:
- “Maybe the journey isn’t so much about becoming anything.
- Maybe it’s about unbecoming everything that isn’t really you,
- so you can be who you were meant to be in the first place”
{wymhacks – Conclusion}
This article summarizes Peter Attia’s “Outlive” but also provides a human biology primer through linked supplementary explanations.
It aims to clarify the book’s key points and enhance understanding of the related biological concepts.
My general takeaways from the book are:
Maximize your Healthspan!
(i.e. Aim to die without having suffered any debilitating chronic disease or ailment)
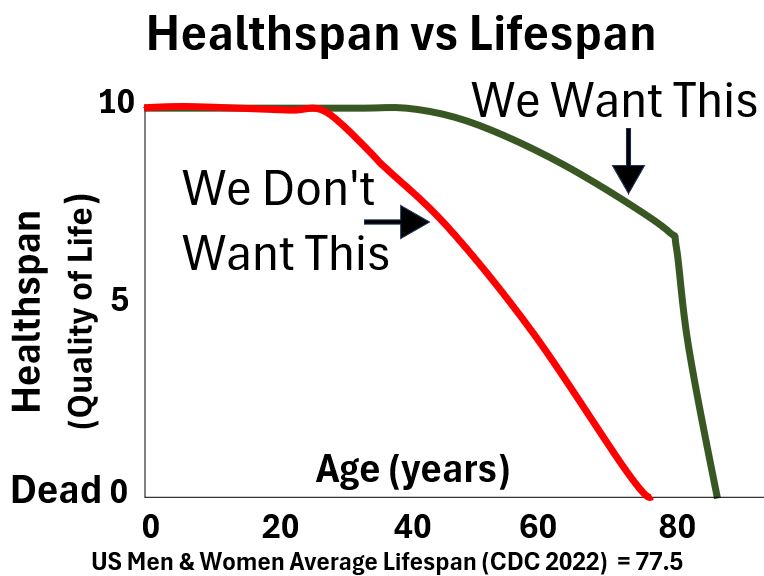
- Be aware of and work on your mental health.
- As you age, it’s even more important that you exercise habitually and comprehensively.
- Work on your balance and stability.
- Exercise to maintain / increase your muscle mass and strength.
- Do long endurance and short high intensity workouts periodically.
- Work on your diet to ensure
- you don’t cause fat spillover into your guts and organs.
- you get enough protein (it’s imperative that you maintain your muscle mass as you age).
- There are no one size fits all dietary or drug / supplement regimes.
- Optimize conditions to get quality sleep (preferably 7.5 to 8.5 hours/day).
- Re Alcohol: Don’t drink at all or minimize alcohol consumption (Ethanol probably causes cancer)
Peter Attia Articles / Podcasts
Explore Attia’s website where you can find articles, podcasts etc. : https://peterattiamd.com/